

Effect of a long-term behavioural weight loss intervention on nephropathy in overweight or obese adults with type 2 diabetes: a secondary analysis of the Look AHEAD randomised clinical trial
- PMID: 25127483
- PMCID: PMC4443484
- DOI: 10.1016/S2213-8587(14)70156-1
Effect of a long-term behavioural weight loss intervention on nephropathy in overweight or obese adults with type 2 diabetes: a secondary analysis of the Look AHEAD randomised clinical trial
Abstract
Background: Long-term effects of behavioural weight loss interventions on diabetes complications are unknown. In a secondary analysis of the Look AHEAD (Action for Health in Diabetes) multicentre randomised clinical trial, we assessed whether an intensive lifestyle intervention (ILI) affects the development of nephropathy in people with type 2 diabetes.
Methods: Overweight or obese people aged 45-76 years with type 2 diabetes were randomly assigned (1:1) to ILI or to a diabetes support and education (DSE) group by a central web-based data management system, stratified by clinical centre and blocked with random block sizes. The ILI was designed to achieve and maintain weight loss through reduced caloric consumption and increased physical activity. The interventions were terminated early because of absence of effect on the primary outcome of cardiovascular disease events in the main Look AHEAD trial. Albuminuria and estimated glomerular filtration rate were prespecified as two of many other outcomes and were assessed from baseline until the interventions ended. They were combined post hoc to define the main outcome for this report, very-high-risk chronic kidney disease (CKD), based on the 2013 Kidney Disease Improving Global Outcomes (KDIGO) classification. Outcomes assessors and laboratory staff were masked to treatment, but participants and interventionists were not masked. Time-to-event data were analysed by intention to treat by the Kaplan-Meier method and proportional hazards models. The Look AHEAD trial is registered with ClinicalTrials.gov, NCT00017953.
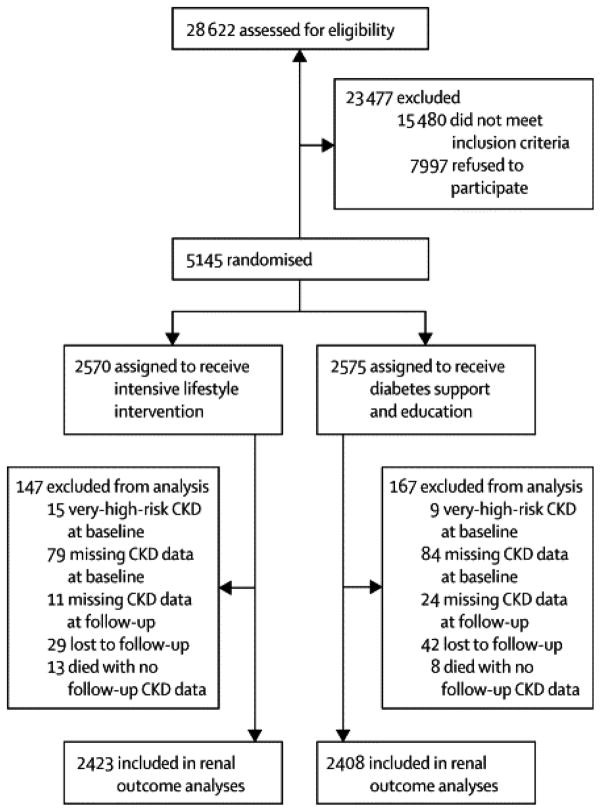
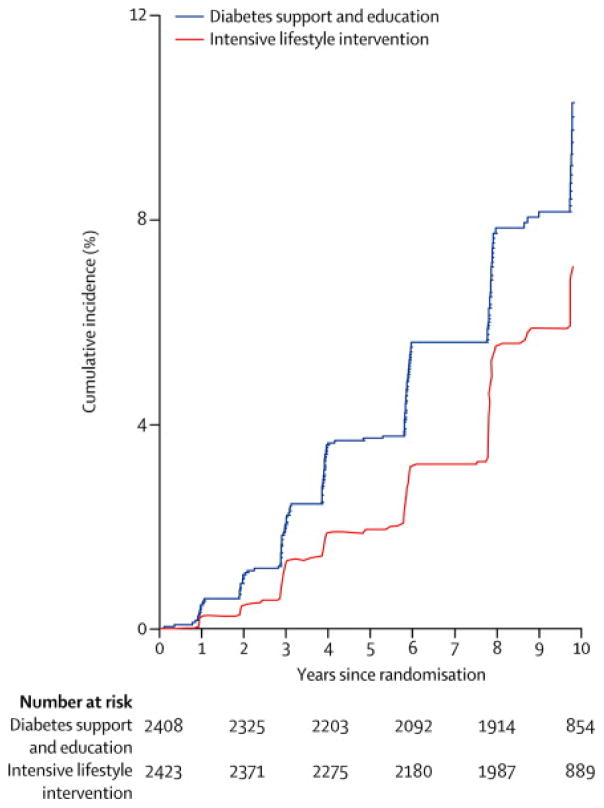
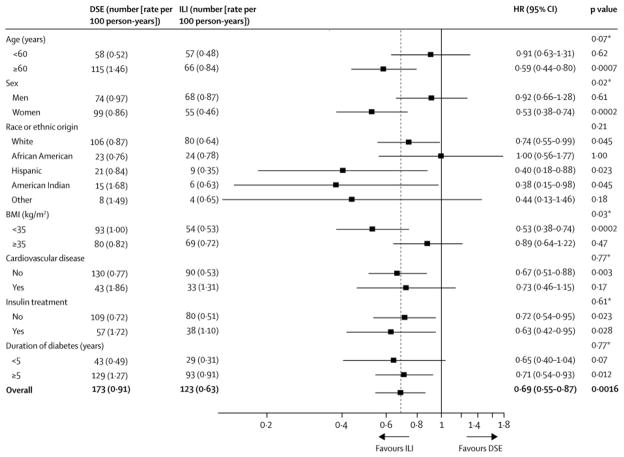
Findings: Of the 5145 participants randomly assigned in the Look AHEAD trial (2570 to ILI and 2575 to DSE), analyses for very-high-risk CKD were done in 2423 (94%) of patients in the ILI group and 2408 (94%) of those in the DSE group. After a median of 8·0 years (IQR 7·9-9·9) of follow-up, the incidence of very-high-risk CKD was lower in the ILI group than in the DSE group, with incidence rates of 0·91 cases per 100 person-years in the DSE group and 0·63 per 100 person-years in the ILI group (difference 0·27 cases per 100 person-years, hazard ratio 0·69, 95% CI 0·55-0·87; p=0·0016). This effect was partly attributable to reductions in bodyweight, HbA1c, and systolic blood pressure. There were no safety concerns regarding kidney-related adverse events.
Interpretation: Weight loss should be considered as an adjunct to medical treatments to prevent or delay progression of CKD in overweight or obese people with type 2 diabetes.
Funding: National Institute of Diabetes and Digestive and Kidney Diseases.
Copyright © 2014 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Do diabetic kidneys deserve a lifestyle change?Lancet Diabetes Endocrinol. 2014 Oct;2(10):769-70. doi: 10.1016/S2213-8587(14)70163-9. Epub 2014 Aug 10. Lancet Diabetes Endocrinol. 2014. PMID: 25127481 No abstract available.
-
Clinical trials: lifestyle intervention reduces CKD risk associated with type 2 diabetes.Nat Rev Nephrol. 2014 Nov;10(11):613. doi: 10.1038/nrneph.2014.166. Epub 2014 Sep 2. Nat Rev Nephrol. 2014. PMID: 25178972 No abstract available.
-
The Look AHEAD study: a missed opportunity.Lancet Diabetes Endocrinol. 2014 Oct;2(10):775-6. doi: 10.1016/S2213-8587(14)70203-7. Lancet Diabetes Endocrinol. 2014. PMID: 25282081 No abstract available.
-
Diabetic kidneys do deserve a lifestyle change.Lancet Diabetes Endocrinol. 2014 Oct;2(10):776. doi: 10.1016/S2213-8587(14)70204-9. Lancet Diabetes Endocrinol. 2014. PMID: 25282082 Free PMC article. No abstract available.
-
The Look AHEAD study: a missed opportunity--authors' reply.Lancet Diabetes Endocrinol. 2014 Oct;2(10):776. doi: 10.1016/S2213-8587(14)70211-6. Lancet Diabetes Endocrinol. 2014. PMID: 25282083 Free PMC article. No abstract available.
References
-
- The DCCT Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977–86. - PubMed
-
- UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33) Lancet. 1998;352:837–53. - PubMed
-
- The ADVANCE Collaborative Group. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008;358:2560–72. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- U01 DK057151/DK/NIDDK NIH HHS/United States
- DK57151/DK/NIDDK NIH HHS/United States
- U01 DK057154/DK/NIDDK NIH HHS/United States
- U01 DK057171/DK/NIDDK NIH HHS/United States
- DK57002/DK/NIDDK NIH HHS/United States
- U01 DK057182/DK/NIDDK NIH HHS/United States
- U01 DK057136/DK/NIDDK NIH HHS/United States
- U01 DK057002/DK/NIDDK NIH HHS/United States
- U01 DK057177/DK/NIDDK NIH HHS/United States
- M01 RR001066/RR/NCRR NIH HHS/United States
- U01 DK057078/DK/NIDDK NIH HHS/United States
- DK57008/DK/NIDDK NIH HHS/United States
- U01 DK057149/DK/NIDDK NIH HHS/United States
- DK57135/DK/NIDDK NIH HHS/United States
- DK57078/DK/NIDDK NIH HHS/United States
- M01RR00211-40/RR/NCRR NIH HHS/United States
- P30 DK048520/DK/NIDDK NIH HHS/United States
- U01 DK057135/DK/NIDDK NIH HHS/United States
- UL1 RR024153/RR/NCRR NIH HHS/United States
- P30 DK046204/DK/NIDDK NIH HHS/United States
- DK57171/DK/NIDDK NIH HHS/United States
- M01 RR002719/RR/NCRR NIH HHS/United States
- DK57131/DK/NIDDK NIH HHS/United States
- M01 RR000056/RR/NCRR NIH HHS/United States
- U01 DK057219/DK/NIDDK NIH HHS/United States
- DK57149/DK/NIDDK NIH HHS/United States
- U01 DK056992/DK/NIDDK NIH HHS/United States
- M01RR01066/RR/NCRR NIH HHS/United States
- DK57182/DK/NIDDK NIH HHS/United States
- DK57178/DK/NIDDK NIH HHS/United States
- P30 DK48520/DK/NIDDK NIH HHS/United States
- U01 DK057131/DK/NIDDK NIH HHS/United States
- M01 RR000051/RR/NCRR NIH HHS/United States
- ImNIH/Intramural NIH HHS/United States
- DK57136/DK/NIDDK NIH HHS/United States
- DK57154/DK/NIDDK NIH HHS/United States
- DK57219/DK/NIDDK NIH HHS/United States
- UL1 TR001082/TR/NCATS NIH HHS/United States
- DK57177/DK/NIDDK NIH HHS/United States
- U01 DK056990/DK/NIDDK NIH HHS/United States
- U01 DK057178/DK/NIDDK NIH HHS/United States
- U01 DK057008/DK/NIDDK NIH HHS/United States
- DK56990/DK/NIDDK NIH HHS/United States
- M01RR02719/RR/NCRR NIH HHS/United States
- M01 RR001346/RR/NCRR NIH HHS/United States
- DK56992/DK/NIDDK NIH HHS/United States
- P30 DK017047/DK/NIDDK NIH HHS/United States
- M01RR00051/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
