

Intensive blood pressure control, falls, and fractures in patients with type 2 diabetes: the ACCORD trial
- PMID: 25127725
- PMCID: PMC4242873
- DOI: 10.1007/s11606-014-2961-3
Intensive blood pressure control, falls, and fractures in patients with type 2 diabetes: the ACCORD trial
Abstract
Background: There are few rigorous studies to confirm or refute the commonly cited concern that control of blood pressure to lower thresholds may result in an increased risk of falls and fractures.
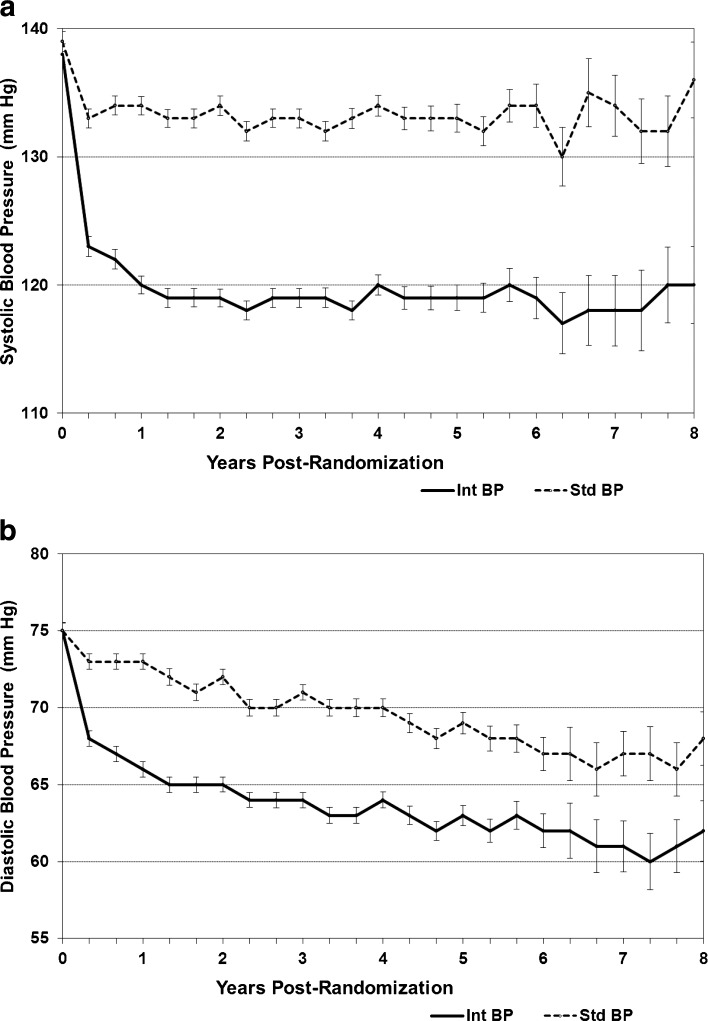
Objective: To compare falls and fractures in participants with type 2 diabetes in the intensive (targeting a systolic blood pressure of < 120 mmHg) and standard (targeting a systolic blood pressure of < 140 mmHg) blood pressure control arms of the Action to Control Cardiovascular Risk in Diabetes (ACCORD) randomized trial (N = 4,733).
Participants: A subset of 3,099 participants self-reported annually on the occurrence of falls and non-spine fractures. Fractures were centrally adjudicated.
Main measures: The incidence of falls in the two treatment groups was compared using a random-effects negative binomial model, and fracture risk was compared using Cox proportional hazards models.
Key results: At enrollment in both groups, the mean age was 62 years, 44% were women, 25% were Black, and mean blood pressure was 138/75 mmHg. During follow-up, all classes of medications, particularly thiazide diuretics, were more commonly prescribed in the intensive group. After 1 year of follow-up, the mean systolic blood pressure was 133 ± 15 mmHg in the standard group and 119 ± 14 mmHg in the intensive group. The adjusted rate of falls did not differ in the intensive and standard groups (62.2/100 person-years vs. 74.1/100 person-years, RR = 0.84, 95% CI 0.54-1.29, p = 0.43). The risk of non-spine fractures was nonsignificantly lower in the intensive than in the standard blood pressure group (HR 0.79, 95% CI 0.62-1.01, p = 0.06).
Conclusions: We conclude that intensive antihypertensive treatment that lowered mean systolic blood pressure to below 120 mmHg was not associated with an increased risk of falls or non-spine fractures in patients age 40 to 79 years with type 2 diabetes.
Trial registration: ClinicalTrials.gov NCT00000620.
Figures


Comment in
-
Hypertension treatment and falls: should we be concerned?J Gen Intern Med. 2014 Dec;29(12):1577-8. doi: 10.1007/s11606-014-3016-5. J Gen Intern Med. 2014. PMID: 25234553 Free PMC article. No abstract available.
-
[Lowering blood pressure without affecting risk of falling].MMW Fortschr Med. 2014 Dec 15;156(21-22):48. doi: 10.1007/s15006-014-3802-3. MMW Fortschr Med. 2014. PMID: 25608402 German. No abstract available.
-
Intensive BP control, falls, and fractures: response to Jolobe (MS #17620).J Gen Intern Med. 2015 May;30(5):547. doi: 10.1007/s11606-015-3191-z. J Gen Intern Med. 2015. PMID: 25650261 Free PMC article. No abstract available.
-
Intensive BP control falls and fractures.J Gen Intern Med. 2015 May;30(5):546. doi: 10.1007/s11606-015-3190-0. J Gen Intern Med. 2015. PMID: 25666211 Free PMC article. No abstract available.
Similar articles
-
Intensive glycemic control is not associated with fractures or falls in the ACCORD randomized trial.Diabetes Care. 2012 Jul;35(7):1525-31. doi: 10.2337/dc11-2184. Diabetes Care. 2012. PMID: 22723583 Free PMC article. Clinical Trial.
-
Intensive BP control falls and fractures.J Gen Intern Med. 2015 May;30(5):546. doi: 10.1007/s11606-015-3190-0. J Gen Intern Med. 2015. PMID: 25666211 Free PMC article. No abstract available.
-
Intensive BP control, falls, and fractures: response to Jolobe (MS #17620).J Gen Intern Med. 2015 May;30(5):547. doi: 10.1007/s11606-015-3191-z. J Gen Intern Med. 2015. PMID: 25650261 Free PMC article. No abstract available.
-
Effects of blood-pressure-lowering treatment on outcome incidence in hypertension: 10 - Should blood pressure management differ in hypertensive patients with and without diabetes mellitus? Overview and meta-analyses of randomized trials.J Hypertens. 2017 May;35(5):922-944. doi: 10.1097/HJH.0000000000001276. J Hypertens. 2017. PMID: 28141660 Review.
-
Effect of intensive lowering of systolic blood pressure treatment on heart failure events: a meta-analysis of randomized controlled studies.J Hum Hypertens. 2019 Sep;33(9):648-657. doi: 10.1038/s41371-019-0221-z. Epub 2019 Jul 30. J Hum Hypertens. 2019. PMID: 31363149
Cited by
-
Short-Term Risk of Serious Fall Injuries in Older Adults Initiating and Intensifying Treatment With Antihypertensive Medication.Circ Cardiovasc Qual Outcomes. 2016 May;9(3):222-9. doi: 10.1161/CIRCOUTCOMES.115.002524. Epub 2016 May 10. Circ Cardiovasc Qual Outcomes. 2016. PMID: 27166208 Free PMC article.
-
Blood Pressure Control Among Older Adults With Hypertension: Narrative Review and Introduction of a Framework for Improving Care.Am J Hypertens. 2021 Apr 2;34(3):258-266. doi: 10.1093/ajh/hpab002. Am J Hypertens. 2021. PMID: 33821943 Free PMC article. Review.
-
Syncope, Hypotension, and Falls in the Treatment of Hypertension: Results from the Randomized Clinical Systolic Blood Pressure Intervention Trial.J Am Geriatr Soc. 2018 Apr;66(4):679-686. doi: 10.1111/jgs.15236. Epub 2018 Mar 30. J Am Geriatr Soc. 2018. PMID: 29601076 Free PMC article. Clinical Trial.
-
Intensive vs Standard Blood Pressure Control and Cardiovascular Disease Outcomes in Adults Aged ≥75 Years: A Randomized Clinical Trial.JAMA. 2016 Jun 28;315(24):2673-82. doi: 10.1001/jama.2016.7050. JAMA. 2016. PMID: 27195814 Free PMC article. Clinical Trial.
-
Preventing Heart Failure by Treating Systolic Hypertension: What Does the SPRINT Add?Curr Hypertens Rep. 2019 Jan 18;21(1):9. doi: 10.1007/s11906-019-0913-3. Curr Hypertens Rep. 2019. PMID: 30659372 Review.
References
-
- Collins R, Peto R, MacMahon S, Hebert P, Fiebach N, Eberlein K, Godwin J, Qizilbash N, Taylor J, Hennekens C. Blood pressure, stroke, and coronary heart disease. Part 2, short-term reductions in blood pressure: overview of randomised drug trials in their epidemiological context. Lancet. 1990;335:827–838. doi: 10.1016/0140-6736(90)90944-Z. - DOI - PubMed
-
- Czernichow S, Zanchetti A, Turnbull F, Barzi F, Ninomiya T, Kengne AP, Lambers Heerspink HJ, Perkovic V, Huxley R, Arima H, Patel A, Chalmers J, Woodward M, MacMahon S, Neal B. The effects of blood pressure reduction and of different blood pressure-lowering regimens on major cardiovascular events according to baseline blood pressure: meta-analysis of randomized trials. J Hypertens. 2011;29(1):4–16. doi: 10.1097/HJH.0b013e32834000be. - DOI - PubMed
-
- Riefkohl EZ, Bieber HL, Burlingame MB, Lowenthal DT. Medications and falls in the elderly: a review of the evidence and practical considerations. Pharm Ther. 2003;28(11):724–733.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
