

The longitudinal effects of physical activity and dietary calcium on bone mass accrual across stages of pubertal development
- PMID: 25130421
- PMCID: PMC4280289
- DOI: 10.1002/jbmr.2319
The longitudinal effects of physical activity and dietary calcium on bone mass accrual across stages of pubertal development
Abstract
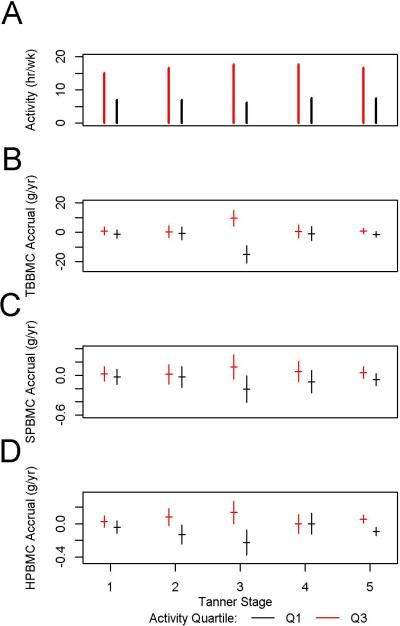
Childhood and adolescence are critical periods of bone mineral content (BMC) accrual that may have long-term consequences for osteoporosis in adulthood. Adequate dietary calcium intake and weight-bearing physical activity are important for maximizing BMC accrual. However, the relative effects of physical activity and dietary calcium on BMC accrual throughout the continuum of pubertal development in childhood remains unclear. The purpose of this study was to determine the effects of self-reported dietary calcium intake and weight-bearing physical activity on bone mass accrual across the five stages of pubertal development in a large, diverse cohort of US children and adolescents. The Bone Mineral Density in Childhood study was a mixed longitudinal study with 7393 observations on 1743 subjects. Annually, we measured BMC by dual-energy X-ray absorptiometry (DXA), physical activity and calcium intake by questionnaire, and pubertal development (Tanner stage) by examination for up to 7 years. Mixed-effects regression models were used to assess physical activity and calcium intake effects on BMC accrual at each Tanner stage. We found that self-reported weight-bearing physical activity contributed to significantly greater BMC accrual in both sexes and racial subgroups (black and nonblack). In nonblack males, the magnitude of the activity effect on total body BMC accrual varied among Tanner stages after adjustment for calcium intake; the greatest difference between high- and low-activity boys was in Tanner stage 3. Calcium intake had a significant effect on bone accrual only in nonblack girls. This effect was not significantly different among Tanner stages. Our findings do not support differential effects of physical activity or calcium intake on bone mass accrual according to maturational stage. The study demonstrated significant longitudinal effects of weight-bearing physical activity on bone mass accrual through all stages of pubertal development.
Keywords: ADOLESCENCE; BONE MASS ACCRUAL; CALCIUM INTAKE; PHYSICAL ACTIVITY; PUBERTY; TANNER STAGE.
© 2014 American Society for Bone and Mineral Research.
Figures

References
-
- Dent C. Problems in metabolic bone disease. Clinical aspects of metabolic bone disease.. Proceedings of the international symposium on clinical aspects of metabolic bone disease; Detroit. 1972; Henry Ford Hospital; pp. 1–7.
-
- Seeman E, Hopper J, Back L, Cooper M, Parkinson E, McKay J, et al. Reduced bone mass in daughters of women with osteoporosis. New Engl J Med. 1989;320:554–8. - PubMed
-
- Sandler R, Slemenda C, LaPorte R, Cauley J, Schramm M, Barresi M, et al. Postmenopausal bone density and milk consumption in childhood and adolescence. Am J Clin Nutr. 1985;42:270–4. - PubMed
-
- NIH Consensus Development Panel on Optimal Calcium Intake. Optimal calcium intake. JAMA. 1994;272(24):1942–8. - PubMed
-
- Matkovic V, Ilich J, Skugor M. Calcium intake and skeletal formation. In: Burchhardt P, Heaney R, editors. Nutritional aspects of osteoporosis '94. Ares-Serono Symposia Pub.; Rome, Italy: 1995. pp. 129–45.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
