

Using surgical appropriateness criteria to examine outcomes of total knee arthroplasty in a United States sample
- PMID: 25132662
- PMCID: PMC4320045
- DOI: 10.1002/acr.22428
Using surgical appropriateness criteria to examine outcomes of total knee arthroplasty in a United States sample
Abstract
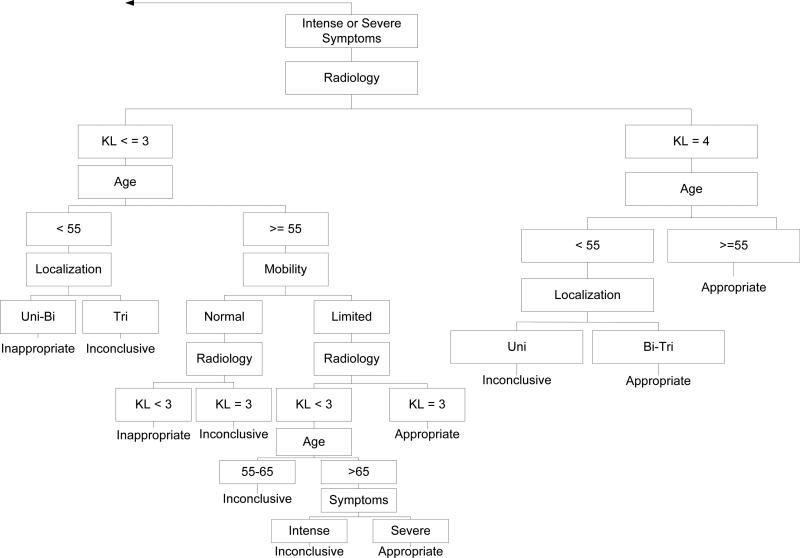
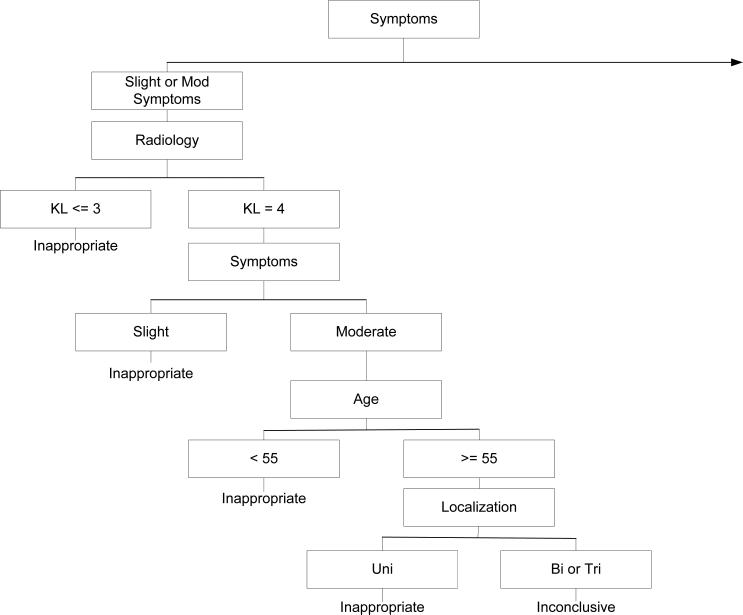
Objective: We determined outcomes for patients classified as appropriate, inconclusive, or inappropriate for total knee arthroplasty (TKA) using a modified version of a validated appropriateness algorithm. Outcome measurement was conceptualized as short-term postoperative change attributable primarily to surgery and rehabilitation (2 months) and as longer-term postoperative change and recovery (1 and 2 years).
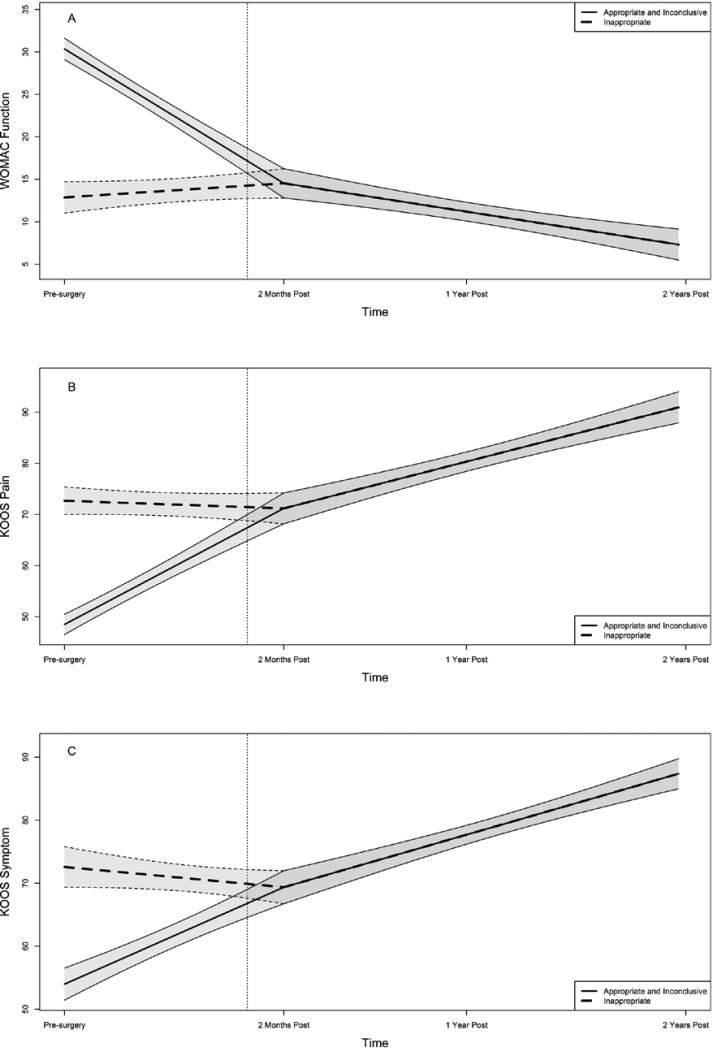
Methods: Preoperative and yearly postoperative Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) function, Knee Injury and Osteoarthritis Outcome Score (KOOS) symptoms and KOOS pain scores were examined for persons undergoing primary TKA in the Osteoarthritis Initiative. Multigroup, 2-piece latent growth curve modeling was used to determine differences in outcome variable changes for each group from presurgery to 2-months postsurgery, as well as over a 2-year postoperative period.
Results: Data from 167 persons with primary TKA were examined. Prevalence rates of appropriate, inconclusive, and inappropriate judgments were 47.9%, 20.8%, and 31.3%, respectively. The inappropriate group showed no change at 2 months following surgery, while appropriate and inconclusive groups had substantial improvement in all outcomes. One-year and 2-year postoperative recovery outcomes were not significantly different among the 3 groups.
Conclusion: The inappropriate group was unchanged 2 months after surgery and on average improved by 2.3 WOMAC function points from presurgery to 1 year following surgery based on our models. Appropriate and inconclusive groups improved by an average of 19.8 WOMAC function points at 1-year postsurgery. These data provide a compelling case for consensus-building efforts to define eligibility criteria for TKA with the goals of reducing variation in patient selection and optimizing both change over time and final outcomes.
Copyright © 2015 by the American College of Rheumatology.
Figures
References
-
- Losina E, Kessler CL, Wright EA, Creel AH, Barrett JA, Fossel AH, et al. Geographic diversity of low-volume hospitals in total knee replacement: implications for regionalization policies. Med Care. 2006;44(7):637–45. - PubMed
-
- Lawson EH, Gibbons MM, Ingraham AM, Shekelle PG, Ko CY. Appropriateness criteria to assess variations in surgical procedure use in the United States. Arch Surg. 2011;146(12):1433–40. - PubMed
-
- Ghomrawi HM, Schackman BR, Mushlin AI. Appropriateness criteria and elective procedures--total joint arthroplasty. N Engl J Med. 2012;367(26):2467–9. - PubMed
-
- Lawson EH, Gibbons MM, Ko CY, Shekelle PG. The appropriateness method has acceptable reliability and validity for assessing overuse and underuse of surgical procedures. J Clin Epidemiol. 2012;65(11):1133–43. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
