

Heart-lung transplantation
- PMID: 25132983
- PMCID: PMC4133550
- DOI: 10.3978/j.issn.2072-1439.2014.05.11
Heart-lung transplantation
Abstract
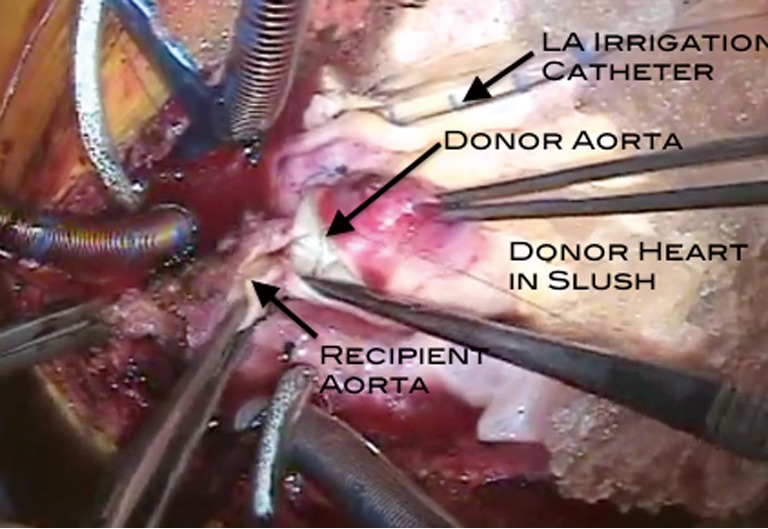
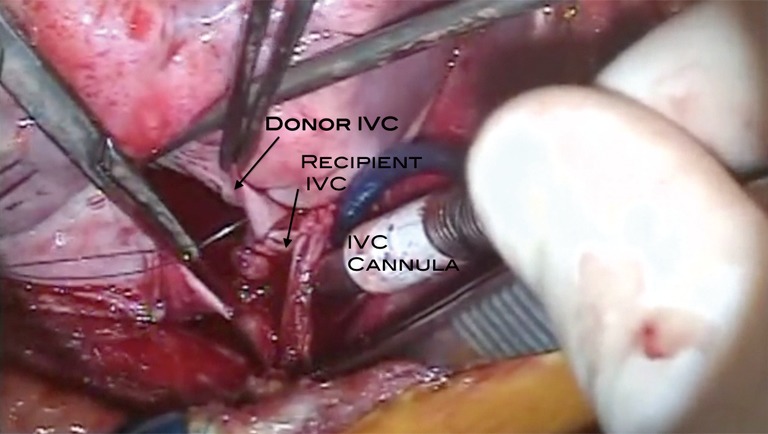
Heart-lung transplantation itself is not a particularly difficult operation technically. It is the setting in which this procedure is performed which is difficult. The three issues of importance in a successful outcome are appropriate harvest of the heart-lung bloc from the donor, careful explant of the heart and lungs of the recipient, and finally the implant of the heart-lung bloc into the recipient. None of this requires extraordinary technical skill, but does require careful coordination and planning as well as adhering to some fundamental principles. One of the major pitfalls encountered is bleeding related to the explant procedure. Another is graft failure related to harvest and/or the implant procedure. The third is injury to either the phrenic nerve(s) or the left recurrent laryngeal nerve related to the explant procedure. Heart-lung transplantation is a major investment in resources of all sorts including financial, personnel, as well as the organs themselves. It is absolutely imperative that this procedure be performed only by experienced surgeons in centers with established expertise.
Keywords: Technique; heart-lung transplantation; transplantation.
Figures
References
-
- Webb WR, Howard HS. Cardio-pulmonary transplantation. Surg Forum 1957;8:313-7 - PubMed
-
- Lower RR, Stofer RC, Hurley EJ, et al. Complete homograft replacement of the heart and both lungs. Surgery 1961;50:842-5 - PubMed
-
- Nakae S, Webb WR, Theodorides T, et al. Respiratory function following cardiopulmonary denervation in dog, cat, and monkey. Surg Gynecol Obstet 1967;125:1285-92 - PubMed
-
- Reitz BA, Burton NA, Jamieson SW, et al. Heart and lung transplantation: autotransplantation and allotransplantation in primates with extended survival. J Thorac Cardiovasc Surg 1980;80:360-72 - PubMed
-
- Reitz BA, Wallwork JL, Hunt SA, et al. Heart-lung transplantation: successful therapy for patients with pulmonary vascular disease. N Engl J Med 1982;306:557-64 - PubMed
LinkOut - more resources
Full Text Sources