

Pathophysiology of fistula formation in Crohn's disease
- PMID: 25133023
- PMCID: PMC4133520
- DOI: 10.4291/wjgp.v5.i3.205
Pathophysiology of fistula formation in Crohn's disease
Abstract
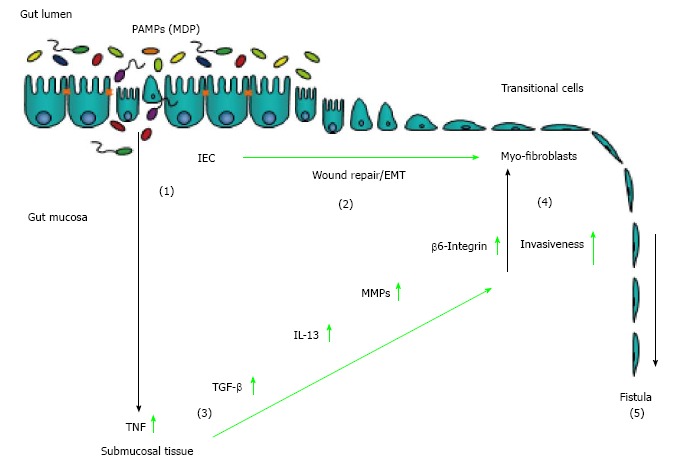
Fistulae represent an important complication in patient suffering from Crohn's disease (CD). Cumulative incidence of fistula formation in CD patients is 17%-50% and about one third of patients suffer from recurring fistulae formation. Medical treatment options often fail and also surgery frequently is not successful. Available data indicate that CD-associated fistulae originate from an epithelial defect that may be caused by ongoing inflammation. Having undergone epithelial to mesenchymal transition (EMT), intestinal epithelial cells (IEC) penetrate into deeper layers of the mucosa and the gut wall causing localized tissue damage formation of a tube like structure and finally a connection to other organs or the body surface. EMT of IEC may be initially aimed to improve wound repair mechanisms since "conventional" wound healing mechanisms, such as migration of fibroblasts, are impaired in CD patients. EMT also enhances activation of matrix remodelling enzymes such as matrix metalloproteinase (MMP)-3 and MMP-9 causing further tissue damage and inflammation. Finally, soluble mediators like TNF and interleukin-13 further induce their own expression in an autocrine manner and enhance expression of molecules associated with cell invasiveness aggravating the process. Additionally, pathogen-associated molecular patterns also seem to play a role for induction of EMT and fistula development. Though current knowledge suggests a number of therapeutic options, new and more effective therapeutic approaches are urgently needed for patients suffering from CD-associated fistulae. A better understanding of the pathophysiology of fistula formation, however, is a prerequisite for the development of more efficacious medical anti-fistula treatments.
Keywords: Crohn’s disease; Epithelial to mesenchymal transition; Fistula; Interleukin-13; Transforming growth factor; Tumor necrosis factor.
Figures
References
-
- Schwartz DA, Loftus EV, Tremaine WJ, Panaccione R, Harmsen WS, Zinsmeister AR, Sandborn WJ. The natural history of fistulizing Crohn’s disease in Olmsted County, Minnesota. Gastroenterology. 2002;122:875–880. - PubMed
-
- Solomon MJ. Fistulae and abscesses in symptomatic perianal Crohn’s disease. Int J Colorectal Dis. 1996;11:222–226. - PubMed
-
- Nielsen OH, Rogler G, Hahnloser D, Thomsen OØ. Diagnosis and management of fistulizing Crohn‘s disease. Nat Clin Pract Gastroenterol Hepatol. 2009;6:92–106. - PubMed
-
- Loftus EV, Schoenfeld P, Sandborn WJ. The epidemiology and natural history of Crohn’s disease in population-based patient cohorts from North America: a systematic review. Aliment Pharmacol Ther. 2002;16:51–60. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
