The association of metacognitive beliefs with emotional distress after diagnosis of cancer
- PMID: 25133826
- PMCID: PMC4321533
- DOI: 10.1037/hea0000096
The association of metacognitive beliefs with emotional distress after diagnosis of cancer
Abstract
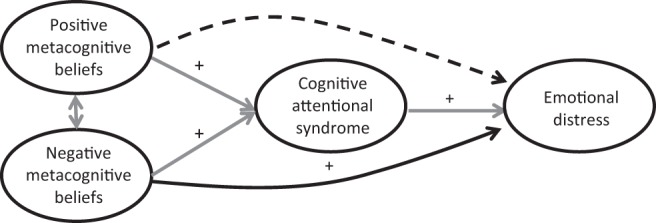
Objective: Emotional distress after a diagnosis of cancer is normal and, for most people, will diminish over time. However, a significant minority of patients with cancer experience persistent or recurrent symptoms of emotional distress for which they need help. A model developed in mental health, the self-regulatory executive function model (S-REF), specifies that maladaptive metacognitive beliefs and processes, including persistent worry, are key to understanding why such emotional problems persist. This cross-sectional study explored, for the first, time whether metacognitive beliefs were associated with emotional distress in a cancer population, and whether this relationship was mediated by worry, as predicted by the S-REF model.
Method: Two hundred twenty-nine participants within 3 months of diagnosis of, and before treatment for, primary breast or prostate cancer completed self-report questionnaires measuring anxiety, depression, posttraumatic stress disorder (PTSD) symptoms, metacognitive beliefs, worry, and illness perceptions.
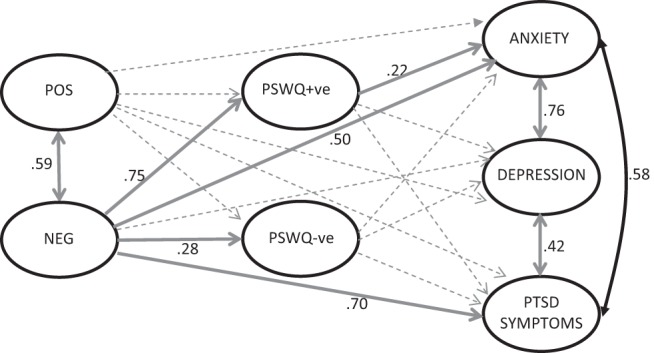
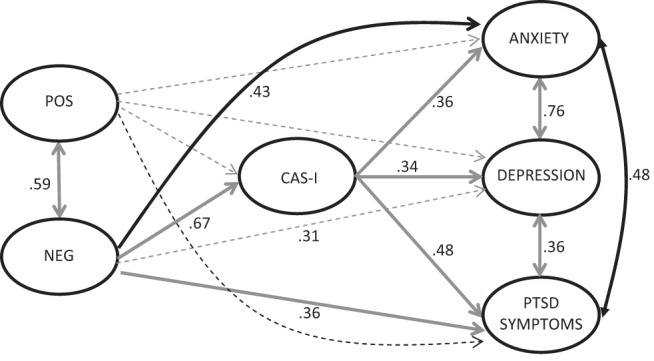
Results: Regression analysis showed that metacognitive beliefs were associated with symptoms of anxiety, depression, and PTSD, and explained additional variance in these outcomes after controlling for age, gender, and illness perceptions. Structural equation modeling was consistent with cross-sectional hypotheses derived from the theory that metacognitive beliefs cause and maintain distress both directly and indirectly by driving worry.
Conclusions: The findings provide promising first evidence that the S-REF model may be usefully applied in cancer. Further study is required to establish the predictive and clinical utility of these findings.
PsycINFO Database Record (c) 2015 APA, all rights reserved.
Figures
References
-
- Andrykowski M. A., & Kangas M. (2010). Posttraumatic stress disorder associated with cancer diagnosis and treatment In Holland J. C., Breitbart W., Jacobsen P. B., Lederberg M. S., Loscalzo M. J., & McCorkle R. (Eds.), Psycho-oncology (pp. 348–357). New York, NY: Oxford University Press. doi:10.1093/med/9780195367430.003.0047 - DOI
-
- Baker P., Beesley H., Dinwoodie R., Fletcher I., Ablett J., Holcombe C., & Salmon P. (2013). “You’re putting thoughts into my head”: A qualitative study of the readiness of patients with breast, lung or prostate cancer to address emotional needs through the first 18 months after diagnosis. Psycho-Oncology, 22, 1402–1410. doi:10.1002/pon.3156 - DOI - PubMed
-
- Brennan J. (2004). Cancer in context: A practical guide to supportive care. Oxford, UK: Oxford University Press.
-
- Brown T. A. (2006). Confirmatory factor analysis for applied research. New York, NY: Guilford Press.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical