

ESRD from autosomal dominant polycystic kidney disease in the United States, 2001-2010
- PMID: 25134777
- PMCID: PMC4396817
- DOI: 10.1053/j.ajkd.2014.05.020
ESRD from autosomal dominant polycystic kidney disease in the United States, 2001-2010
Abstract
Background: Autosomal dominant polycystic kidney disease (ADPKD) is amenable to early detection and specialty care. Thus, while important to patients with the condition, end-stage renal disease (ESRD) from ADPKD also may be an indicator of the overall state of nephrology care.
Study design: Retrospective cohort study of temporal trends in ESRD from ADPKD and pre-renal replacement therapy (RRT) nephrologist care, 2001-2010 (n = 23,772).
Setting & participants: US patients who initiated maintenance RRT from 2001 through 2010 (n = 1,069,343) from US Renal Data System data.
Predictor: ESRD from ADPKD versus from other causes for baseline characteristics and clinical outcomes; interval 2001-2005 versus 2006-2010 for comparisons of cohort of patients with ESRD from ADPKD.
Outcomes: Death, wait-listing for kidney transplant, kidney transplantation.
Measurements: US census data were used as population denominators. Poisson distribution was used to compute incidence rates (IRs). Incidence ratios were standardized to rates in 2001-2002 for age, sex, and race/ethnicity. Patients with and without ADPKD were matched to compare clinical outcomes. Poisson regression was used to calculate IRs and adjusted HRs for clinical events after inception of RRT.
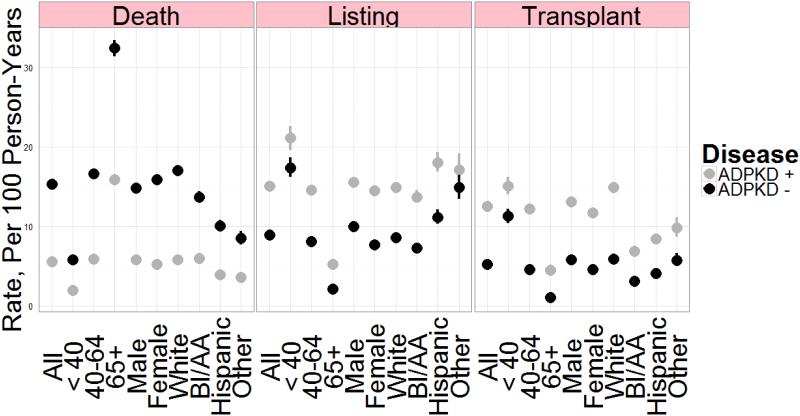
Results: General population incidence ratios in 2009-2010 were unchanged from 2001-2002 (incidence ratio, 1.02). Of patients with ADPKD, 48.1% received more than 12 months of nephrology care before RRT; preemptive transplantation was the initial RRT in 14.3% and fistula was the initial hemodialysis access in 35.8%. During 4.9 years of follow-up, patients with ADPKD were more likely to be listed for transplantation (IR, 11.7 [95% CI, 11.5-12.0] vs 8.4 [95% CI, 8.2-8.7] per 100 person-years) and to undergo transplantation (IR, 9.8 [95% CI, 9.5-10.0] vs 4.8 [95% CI, 4.7-5.0] per 100 person-years) and less likely to die (IR, 5.6 [95% CI, 5.4-5.7] vs 15.5 [95% CI, 15.3-15.8] per 100 person-years) than matched controls without ADPKD.
Limitations: Retrospective nonexperimental registry-based study of associations; cause-and-effect relationships cannot be determined.
Conclusions: Although outcomes on dialysis therapy are better for patients with ADPKD than for those without ADPKD, access to predialysis nephrology care and nondeclining ESRD rates may be a cause for concern.
Keywords: Dialysis; autosomal dominant polycystic kidney disease (ADPKD); clinical outcome; end-stage renal disease (ESRD); incidence; registry data; renal replacement therapy (RRT); renal transplant.
Copyright © 2014 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Collins AJ, Foley RN, Herzog C, et al. U.S. Renal Data System 2012 Annual Data Report. Am J Kidney Dis. 2013;61:A7. e1-A7,476. - PubMed
-
- Jouret F, Krzesinski JM. Tolvaptan in autosomal dominant polycystic kidney disease. N Engl J Med. 2013;368:1258–1259. - PubMed
-
- Stallone G, Infante B, Grandaliano G, et al. Rapamycin for treatment of type I autosomal dominant polycystic kidney disease (RAPYD-study): a randomized, controlled study. Nephrol Dial Transplant. 2012;27:3560–3567. - PubMed
-
- U.S. Renal Data System Researcher's Guide to the USRDS Database; Appendix D: Data File Descriptions. 2013 Available at: http://www.usrds.org/2013/rg/C_Data_File_Descriptions_13.pdf. Accessed May 20, 2014.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
