

Multidisciplinary intensive education in the hospital improves outcomes for hospitalized heart failure patients in a Japanese rural setting
- PMID: 25134951
- PMCID: PMC4141092
- DOI: 10.1186/1472-6963-14-351
Multidisciplinary intensive education in the hospital improves outcomes for hospitalized heart failure patients in a Japanese rural setting
Abstract
Background: Heart failure (HF) patients living in rural areas have a lack of HF knowledge and poor self-care because of limited medical care access. Multidisciplinary education to improve self-care behavior is indispensable for such patients. The present study evaluated whether intensive inpatient education improved outcomes of hospitalized HF patients in a Japanese rural setting.
Methods: An inpatient HF management program based on multidisciplinary team intervention was applied to hospitalized HF patients in a Japanese rural area. We defined patients treated within the program from May 2009 to April 2011 as the intervention group (n = 144), and those treated with the usual care from May 2006 to April 2009 as the usual care group (n = 133). The composite endpoints of HF hospitalization and all-cause mortality were compared between the two groups.
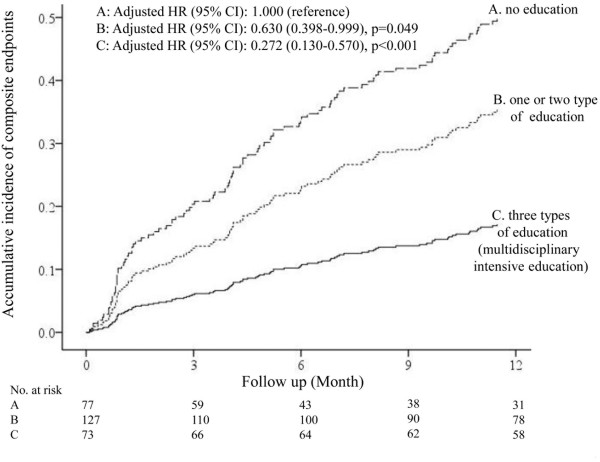
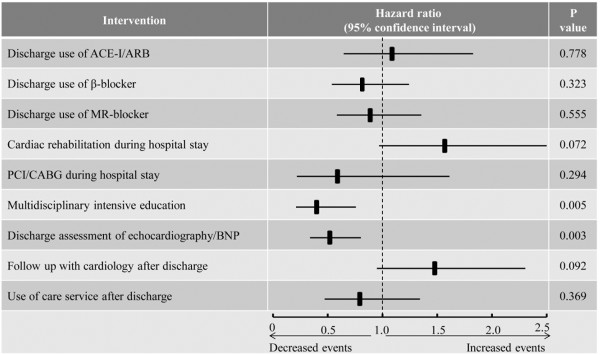
Results: Compared with patients in the usual care group, those in the intervention group more often received the optimal interventions such as discharge use of β-blockers, cardiac rehabilitation, pre-discharge diagnostic tests, and multidisciplinary intensive education including nurse-led patient education, pharmacist's medication teaching, and dietitian's nutritional guidance (all P < 0.05). The incidence of the composite endpoints significantly decreased after introducing the program (P < 0.001). Among a number of interventions, multidisciplinary intensive education was the most effective intervention to improve the primary outcome (P < 0.001).
Conclusions: Multidisciplinary intensive education is a key strategy for helping improve the outcome for Japanese HF patients in a rural setting. Our data may give a positive impact on the improvement of healthcare system in Japan.
Figures



References
-
- Jaarsma T, Beattie JM, Ryder M, Rutten FH, McDonagh T, Mohacsi P, Murray SA, Grodzicki T, Bergh I, Metra M, Ekman I, Angermann C, Leventhal M, Pitsis A, Anker SD, Gavazzi A, Ponikowski P, Dickstein K, Delacretaz E, Blue L, Strasser F, McMurray J, Advanced Heart Failure Study Group of the HFA of the ESC Palliative care in heart failure: a position statement from the palliative care workshop of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2009;11:433–443. doi: 10.1093/eurjhf/hfp041. - DOI - PubMed
-
- McAlister FA, Stewart S, Ferrua S, McMurray JJ. Multidisciplinary strategies for the management of heart failure patients at high risk for admission: a systematic review of randomized trials. J Am Coll Cardiol. 2004;44:810–819. - PubMed
-
- Gonseth J, Guallar-Castillón P, Banegas JR, Rodríguez-Artalejo F. The effectiveness of disease management programmes in reducing hospital re-admission in older patients with heart failure: a systematic review and meta-analysis of published reports. Eur Heart J. 2004;18:1570–1595. doi: 10.1016/j.ehj.2004.04.022. - DOI - PubMed
Pre-publication history
-
- The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1472-6963/14/351/prepub
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
