

Setting thresholds to varying blood pressure monitoring intervals differentially affects risk estimates associated with white-coat and masked hypertension in the population
- PMID: 25135185
- PMCID: PMC4420482
- DOI: 10.1161/HYPERTENSIONAHA.114.03614
Setting thresholds to varying blood pressure monitoring intervals differentially affects risk estimates associated with white-coat and masked hypertension in the population
Abstract
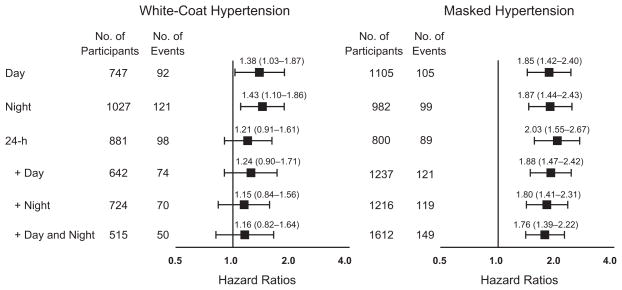
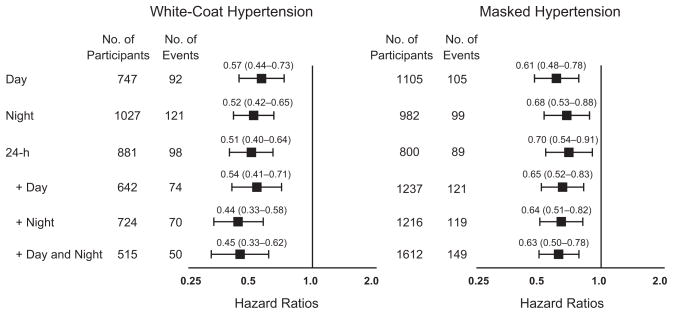
Outcome-driven recommendations about time intervals during which ambulatory blood pressure should be measured to diagnose white-coat or masked hypertension are lacking. We cross-classified 8237 untreated participants (mean age, 50.7 years; 48.4% women) enrolled in 12 population studies, using ≥140/≥90, ≥130/≥80, ≥135/≥85, and ≥120/≥70 mm Hg as hypertension thresholds for conventional, 24-hour, daytime, and nighttime blood pressure. White-coat hypertension was hypertension on conventional measurement with ambulatory normotension, the opposite condition being masked hypertension. Intervals used for classification of participants were daytime, nighttime, and 24 hours, first considered separately, and next combined as 24 hours plus daytime or plus nighttime, or plus both. Depending on time intervals chosen, white-coat and masked hypertension frequencies ranged from 6.3% to 12.5% and from 9.7% to 19.6%, respectively. During 91 046 person-years, 729 participants experienced a cardiovascular event. In multivariable analyses with normotension during all intervals of the day as reference, hazard ratios associated with white-coat hypertension progressively weakened considering daytime only (1.38; P=0.033), nighttime only (1.43; P=0.0074), 24 hours only (1.21; P=0.20), 24 hours plus daytime (1.24; P=0.18), 24 hours plus nighttime (1.15; P=0.39), and 24 hours plus daytime and nighttime (1.16; P=0.41). The hazard ratios comparing masked hypertension with normotension were all significant (P<0.0001), ranging from 1.76 to 2.03. In conclusion, identification of truly low-risk white-coat hypertension requires setting thresholds simultaneously to 24 hours, daytime, and nighttime blood pressure. Although any time interval suffices to diagnose masked hypertension, as proposed in current guidelines, full 24-hour recordings remain standard in clinical practice.
Keywords: ambulatory blood pressure monitoring; cardiovascular risk; masked hypertension; population science; white-coat hypertension.
© 2014 American Heart Association, Inc.
Figures
References
-
- National Institute for Health and Clinical Excellence (NICE) The Clinical Management of Primary Hypertension in Adults. UK: National Clinical Guideline Centre; 2011.
-
- O’Brien E, Parati G, Stergiou G, et al. European Society of Hypertension Working Group on Blood Pressure Monitoring. European Society of Hypertension position paper on ambulatory blood pressure monitoring. J Hypertens. 2013;31:1731–1767. - PubMed
-
- Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jr, Jones DW, Materson BJ, Oparil S, Wright JT, Jr, Roccella EJ Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. National Heart, Lung, and Blood Institute; National High Blood Pressure Education Program Coordinating Committee. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003;42:1206–1252. - PubMed
-
- Ogihara T, Kikuchi K, Matsuoka H, et al. Japanese Society of Hypertension Committee. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2009) Hypertens Res. 2009;32:3–107. - PubMed
-
- Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC) Eur Heart J. 2013;34:2159–2219. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
