

Ivabradine Versus Beta-Blockers in Patients with Conduction Abnormalities or Left Ventricular Dysfunction Undergoing Cardiac Surgery
- PMID: 25135587
- PMCID: PMC4265234
- DOI: 10.1007/s40119-013-0024-1
Ivabradine Versus Beta-Blockers in Patients with Conduction Abnormalities or Left Ventricular Dysfunction Undergoing Cardiac Surgery
Abstract
Introduction: In patients with conduction abnormalities or left ventricle (LV) dysfunction the use of β-blockers for post cardiac surgery rhythm control is difficult and controversial, with a paucity of information about other drugs such ivabradine used postoperatively. The objective of this study was to compare the efficacy and safety of ivabradine versus metoprolol used perioperatively in cardiac surgery patients with conduction abnormalities or LV systolic dysfunction.
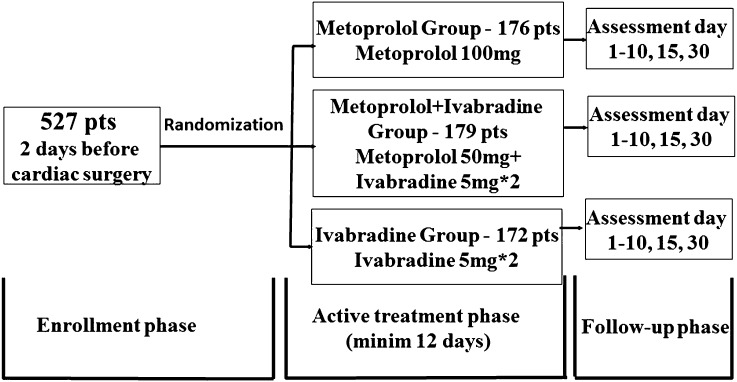
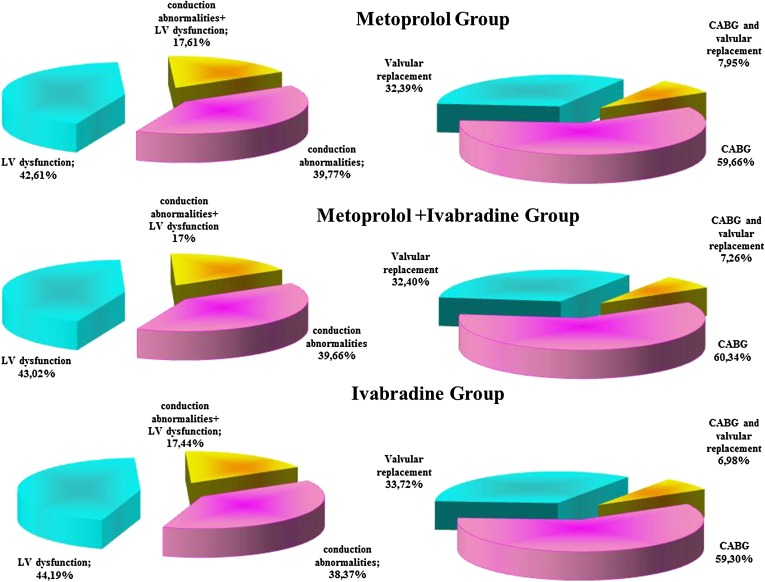
Methods: This was an open-label, randomized clinical trial enrolling 527 patients with conduction abnormalities or LV systolic dysfunction undergoing coronary artery bypass grafting or valvular replacement, randomized to take ivabradine or metoprolol, or metoprolol plus ivabradine. The primary endpoints were the composites of 30-day mortality, in-hospital atrial fibrillation (AF), in-hospital three-degree atrioventricular block and need for pacing, in-hospital worsening heart failure (HF; safety endpoints), duration of hospital stay and immobilization and the above endpoint plus in-hospital bradycardia, gastrointestinal symptoms, sleep disturbances, cold extremities (efficacy plus safety endpoint).
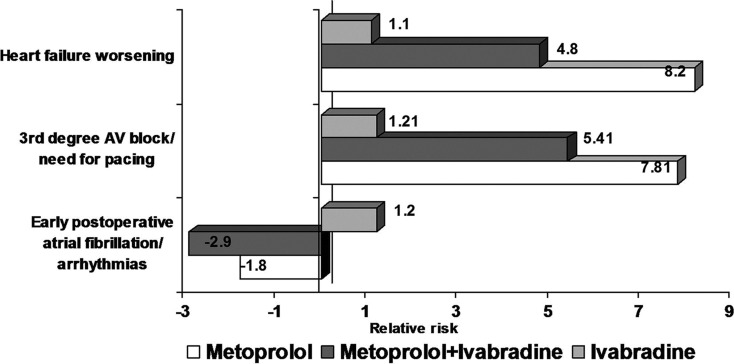
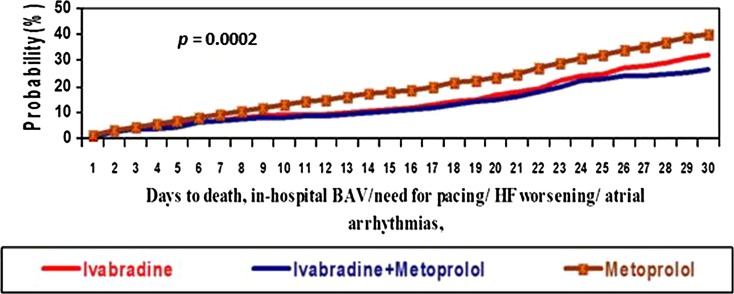
Results: Heart rate reduction and prevention of postoperative AF or tachyarrhythmia with combined therapy was more effective than with metoprolol or ivabradine alone during the immediate postoperative management of cardiac surgery patients. In the Ivabradine group, the frequency of early postoperative pacing and HF worsening was smaller than in the Metoprolol group and in combined therapy group. The frequency of primary combined endpoint was lower in the combined Ivabradine + Metoprolol group compared with the monotherapy groups.
Conclusion: Considering efficacy and safety, the cardiac rhythm reduction after open heart surgery in patients with conduction abnormalities or LV dysfunction with ivabradine plus metoprolol emerged as the best treatment in this trial.
Keywords: Atrial fibrillation; Beta-blocker; Cardiac surgery; Cardiology; Coronary artery bypass surgery; Ivabradine; Metoprolol; Postoperative arrhythmias; Valvular replacement.
Figures
Similar articles
-
Prevention of perioperative atrial fibrillation with betablockers in coronary surgery: betaxolol versus metoprolol.Interact Cardiovasc Thorac Surg. 2009 Jul;9(1):89-93. doi: 10.1510/icvts.2009.202465. Epub 2009 Apr 16. Interact Cardiovasc Thorac Surg. 2009. PMID: 19372098 Clinical Trial.
-
Short-Term Results of Ivabradine versus Metoprolol: The Effects on Atrial Fibrillation in Patients Undergoing Off-Pump Coronary Artery Bypass Grafting.Braz J Cardiovasc Surg. 2022 Dec 1;37(6):857-865. doi: 10.21470/1678-9741-2021-0201. Braz J Cardiovasc Surg. 2022. PMID: 35244381 Free PMC article.
-
Comparative effectiveness of metoprolol, ivabradine, and its combination in the management of inappropriate sinus tachycardia in coronary artery bypass graft patients.Indian J Pharmacol. 2021 Jul-Aug;53(4):264-269. doi: 10.4103/ijp.IJP_478_19. Indian J Pharmacol. 2021. PMID: 34414903 Free PMC article. Clinical Trial.
-
Impact of ivabradine on the cardiac function of chronic heart failure reduced ejection fraction: Meta-analysis of randomized controlled trials.Clin Cardiol. 2021 Apr;44(4):463-471. doi: 10.1002/clc.23581. Epub 2021 Feb 27. Clin Cardiol. 2021. PMID: 33638556 Free PMC article. Review.
-
Perioperative beta-blockers for preventing surgery-related mortality and morbidity in adults undergoing cardiac surgery.Cochrane Database Syst Rev. 2019 Sep 23;9(9):CD013435. doi: 10.1002/14651858.CD013435. Cochrane Database Syst Rev. 2019. PMID: 31544227 Free PMC article.
Cited by
-
Ginseng Radix et Rhizoma enhanced the effect of metoprolol in chronic heart failure by inhibiting autophagy in male C57BL/6J mice.PLoS One. 2024 Aug 14;19(8):e0301875. doi: 10.1371/journal.pone.0301875. eCollection 2024. PLoS One. 2024. PMID: 39141645 Free PMC article.
-
Ivabradine as adjuvant treatment for chronic heart failure.Cochrane Database Syst Rev. 2020 Nov 4;11(11):CD013004. doi: 10.1002/14651858.CD013004.pub2. Cochrane Database Syst Rev. 2020. PMID: 33147368 Free PMC article.
-
Ivabradine: pre-clinical and clinical evidence in the setting of ventricular arrhythmias.Hippokratia. 2022 Apr-Jun;26(2):49-54. Hippokratia. 2022. PMID: 37188047 Free PMC article. Review.
-
Ivabradine and AF: Coincidence, Correlation or a New Treatment?Arrhythm Electrophysiol Rev. 2020 Feb 12;8(4):300-303. doi: 10.15420/aer.2019.30.2. Arrhythm Electrophysiol Rev. 2020. PMID: 32685161 Free PMC article. Review.
-
Postoperative atrial fibrillation after off-pump coronary artery bypass grafting.Indian J Thorac Cardiovasc Surg. 2020 May;36(3):259. doi: 10.1007/s12055-020-00952-x. Epub 2020 Apr 8. Indian J Thorac Cardiovasc Surg. 2020. PMID: 33061138 Free PMC article. No abstract available.
References
-
- Mina K, Chung MD. Cardiac surgery: postoperative arrhythmias. Crit Care Med. 2000;28(10 Suppl):N136–44. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
