

Brain pathology contributes to simultaneous change in physical frailty and cognition in old age
- PMID: 25136002
- PMCID: PMC4296120
- DOI: 10.1093/gerona/glu117
Brain pathology contributes to simultaneous change in physical frailty and cognition in old age
Abstract
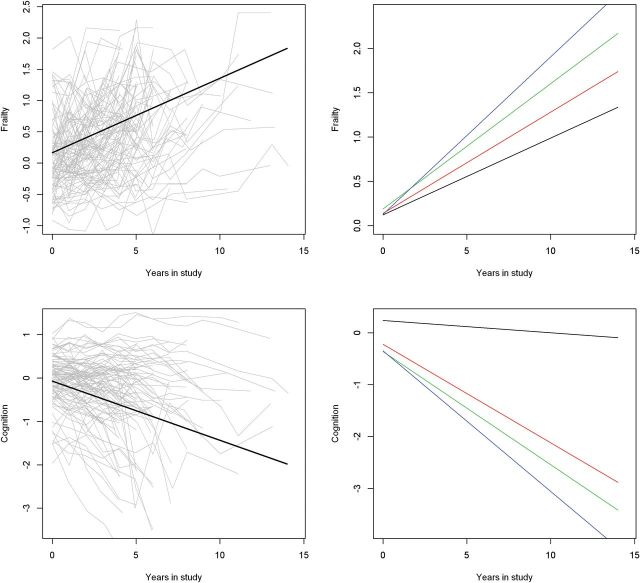
Objective: First, we tested the hypothesis that the rate of change of physical frailty and cognitive function in older adults are correlated. Next, we examined if their rates of change are associated with the same brain pathologies.
Methods: About 2,167 older adults participating in the Religious Orders Study and the Rush Memory and Aging Project had annual clinical evaluations. Bivariate random coefficient models were used to estimate simultaneously the rates of change in both frailty and cognition, and the correlation of change was characterized by a joint distribution of the random effects. Then, we examined whether postmortem indices from deceased were associated with the rate of change of frailty and cognition.
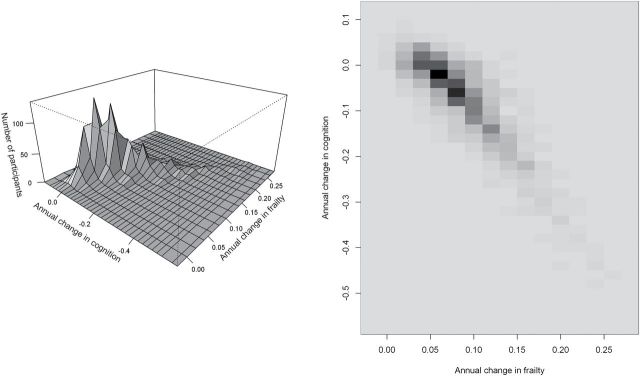
Results: During an average follow-up of 6 years, frailty worsened by 0.09 unit/y and cognition declined by 0.08 unit/y. Most individuals showed worsening frailty and cognition (82.8%); 17% showed progressive frailty alone and <1% showed only cognitive decline. The rates of change of frailty and cognition were strongly correlated (ρ = -0.73, p < .001). Among deceased (N = 828), Alzheimer's disease pathology, macroinfarcts, and nigral neuronal loss showed independent associations with the rate of change in both frailty and cognition (all ps < .001). In these models, demographics explained about 9% of the variation in individual rate of change in frailty, and neuropathologies explained about 8%. In contrast, demographics and neuropathologies accounted for 2% and 30%, respectively, of the variance in the cognitive decline.
Conclusion: The rates of change in frailty and cognition are strongly correlated and this may be due in part because they share a common pathologic basis.
Keywords: Aging; Brain pathology.; Cognition; Physical frailty.
© The Author 2014. Published by Oxford University Press on behalf of The Gerontological Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Jack CR, Jr, Albert M, Knopman DS, et al. Introduction to revised criteria for the diagnosis of Alzheimer’s disease: National Institute on Aging and the Alzheimer’s Association workgroup. Alzheimers Dement. 2011;7:256–262.
-
- Lang AE. A critical appraisal of the premotor symptoms of Parkinson’s disease: potential usefulness in early diagnosis and design of neuroprotective trials.Mov Disord. 2011;26:775–783. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
