Management of infantile hemangiomas: current trends
- PMID: 25136206
- PMCID: PMC4134656
- DOI: 10.4103/0974-2077.138324
Management of infantile hemangiomas: current trends
Abstract
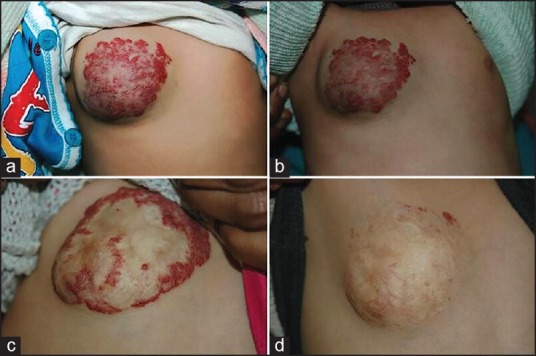
Infantile hemangiomas (IH) are common vascular tumours. IH have a characteristic natural course. They proliferate rapidly during the early infantile period followed by a period of gradual regression over several years. Most of the uncomplicated IH undergo spontaneous involution, with a small proportion of cases requiring intervention. These are children with IH in life-threatening locations, local complications like haemorrhage, ulceration and necrosis and functional or cosmetic disfigurements. Systemic corticosteroids have been the first line of treatment for many years. Recently, non-selective beta-blockers, such as oral propranalol and topical timolol, have emerged as promising and safer therapies. Other treatment options include interferon α and vincristine which are reserved for life-threatening haemangiomas that are unresponsive to conventional therapy. This review mainly focuses on the current trends and evidence-based approach in the management of IH.
Keywords: Infantile hemangioma; propranolol; pulsed dye laser; steroids; timolol.
Conflict of interest statement
Figures



References
-
- Li J, Chen X, Zhao S, Hu X, Chen C, Ouyang F, et al. Demographic and clinical characteristics and risk factors for infantile hemangioma: A Chinese case-control study. Arch Dermatol. 2011;147:1049–56. - PubMed
-
- Kilcline C, Frieden IJ. Infantile hemangiomas: How common are they. A systematic review of the medical literature? Pediatr Dermatol. 2008;25:168–73. - PubMed
-
- Chang LC, Haggstrom AN, Drolet BA, Baselga E, Chamlin SL, Garzon MC, et al. Hemangioma Investigator Group. Growth characteristics of infantile hemangiomas: Implications for management. Pediatrics. 2008;122:360–7. - PubMed
-
- Haggstrom AN, Drolet BA, Baselga E, Chamlin SL, Garzon MC, Horii KA, et al. Prospective study of infantile hemangiomas: Clinical characteristics predicting complications and treatment. Pediatrics. 2006;118:882–7. - PubMed
-
- Metry DW, Hawrot A, Altman C, Frieden IJ. Association of solitary, segmental hemangiomas of the skin with visceral hemangiomatosis. Arch Dermatol. 2004;140:591–6. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources