Rapid regression of choroidal metastasis from lung cancer using erlotinib (Tarceva)
- PMID: 25136232
- PMCID: PMC4134551
- DOI: 10.4103/0974-620X.137159
Rapid regression of choroidal metastasis from lung cancer using erlotinib (Tarceva)
Abstract
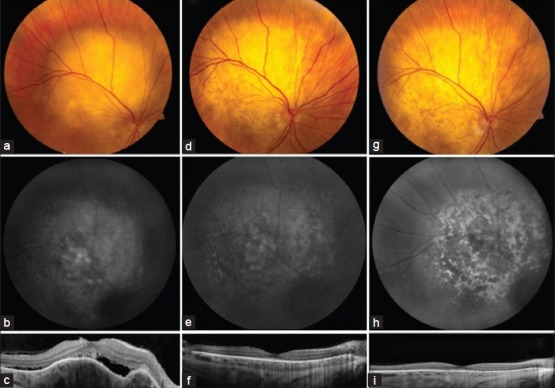
Lung carcinoma is the leading cause of cancer-related deaths and is the primary source for choroidal metastasis in over 20% cases. Non-small-cell lung cancer (NSCLC) accounts for 85% of all lung cancer cases. Patients with metastatic NSCLC have a median survival of one year. Successful treatment of systemic metastasis from NSCLC using erlotinib has been documented. The effect of oral erlotinib on choroidal metastasis has been rarely reported. We document a case and study the effect of oral erlotinib on choroidal metastasis from NSCLC. A 48-year-old Caucasian female presented with biopsy-proven primary NSCLC with systemic metastasis and solitary choroidal metastasis of 4.8 mm thickness in the right eye. The patient was treated with 100 mg daily dose of oral erlotinib. Two weeks after starting erlotinib therapy, the patient showed complete regression of choroidal metastasis to a flat scar with resolution of subretinal fluid and improvement of visual acuity from 20/100 to 20/25. There was no evidence of recurrence at five-month follow-up. Erlotinib is an alternative therapy for choroidal metastasis from NSCLC.
Keywords: Choroidal metastasis; erlotinib; lung cancer; non-small-cell lung cancer.
Conflict of interest statement
Figures
References
-
- Siege R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29. - PubMed
-
- Shields CL, Shields JA, Gross NE, Schwartz GP, Lally SE. Survey of 520 eyes with uveal metastases. Ophthalmology. 1997;104:1265–76. - PubMed
-
- Cataldo VD, Gibbons DL, Perez-Soler R, Quintas-Cardama A. Treatment of non-small-cell lung cancer with erlotinib or gefitinib. N Eng J Med. 2011;364:947–55. - PubMed
-
- Weber B, Sorensen BS, Knap MM, Madsen HH, Nexo E, Meldgaard P. Complete pathologic response in lung tumors in two patients with metastatic non-small cell lung cancer treated with erlotinib. J Thorac Oncol. 2011;6:1946–9. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources