

Management of carotid artery trauma
- PMID: 25136406
- PMCID: PMC4130758
- DOI: 10.1055/s-0034-1372521
Management of carotid artery trauma
Abstract
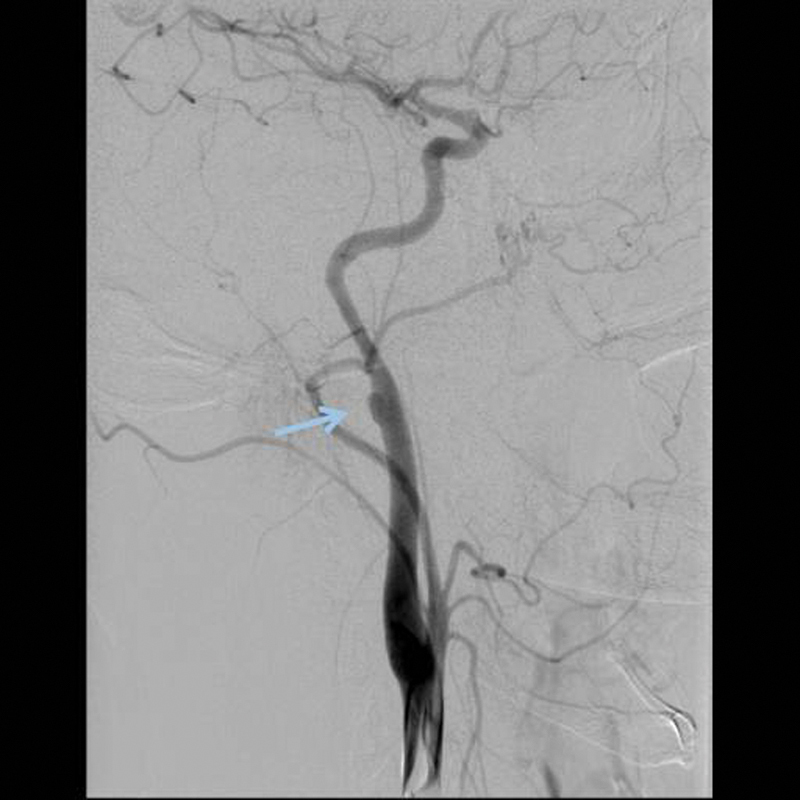
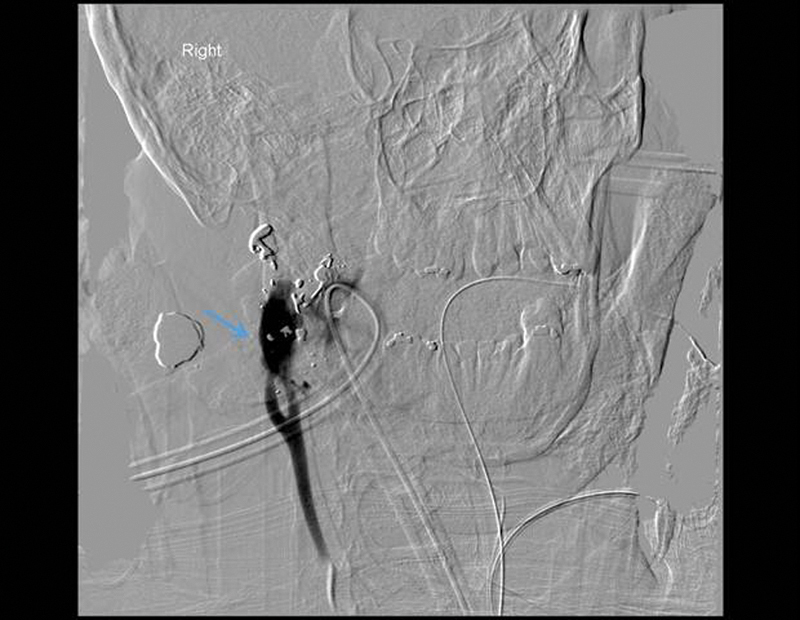
With increased awareness and liberal screening of trauma patients with identified risk factors, recent case series demonstrate improved early diagnosis of carotid artery trauma before they become problematio. There remains a need for unified screening criteria for both intracranial and extracranial carotid trauma. In the absence of contraindications, antithrombotic agents should be considered in blunt carotid artery injuries, as there is a significant risk of progression of vessel injury with observation alone. Despite CTA being used as a common screening modality, it appears to lack sufficient sensitivity. DSA remains to be the gold standard in screening. Endovascular techniques are becoming more widely accepted as the primary surgical modality in the treatment of blunt extracranial carotid injuries and penetrating/blunt intracranial carotid lessions. Nonetheless, open surgical approaches are still needed for the treatment of penetrating extracranial carotid injuries and in patients with unfavorable lesions for endovascular intervention.
Keywords: blunt carotid artery trauma; endovascular repair; extracranial carotid artery trauma; internal carotid artery; intracranial cartoid artery trauma; open repair; penetrating carotid artery trauma.
Figures

References
-
- Kraus R R, Bergstein J M, DeBord J R. Diagnosis, treatment, and outcome of blunt carotid arterial injuries. Am J Surg. 1999;178(3):190–193. - PubMed
-
- Biousse V, D'Anglejan-Chatillon J, Touboul P J, Amarenco P, Bousser M G. Time course of symptoms in extracranial carotid artery dissections. A series of 80 patients. Stroke. 1995;26(2):235–239. - PubMed
-
- Dua A, Desai S S, Kuy S. et al. Predicting outcomes using the National Trauma Data Bank: optimum management of traumatic blunt carotid and blunt thoracic injury. Perspect Vasc Surg Endovasc Ther. 2012;24(3):123–127. - PubMed
-
- Schneidereit N P Simons R Nicolaou S et al. Utility of screening for blunt vascular neck injuries with computed tomographic angiography J Trauma 2006601209–215., discussion 215–216 - PubMed
-
- Cogbill T H, Moore E E, Meissner M. et al. The spectrum of blunt injury to the carotid artery: a multicenter perspective. J Trauma. 1994;37(3):473–479. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources