

The free caesareans policy in low-income settings: an interrupted time series analysis in Mali (2003-2012)
- PMID: 25137072
- PMCID: PMC4138145
- DOI: 10.1371/journal.pone.0105130
The free caesareans policy in low-income settings: an interrupted time series analysis in Mali (2003-2012)
Abstract
Introduction: Several countries have instituted fee exemptions for caesareans to reduce maternal and newborn mortality.
Objectives: To evaluate the effect of fee exemptions for caesareans on population caesarean rates taking into account different levels of accessibility.
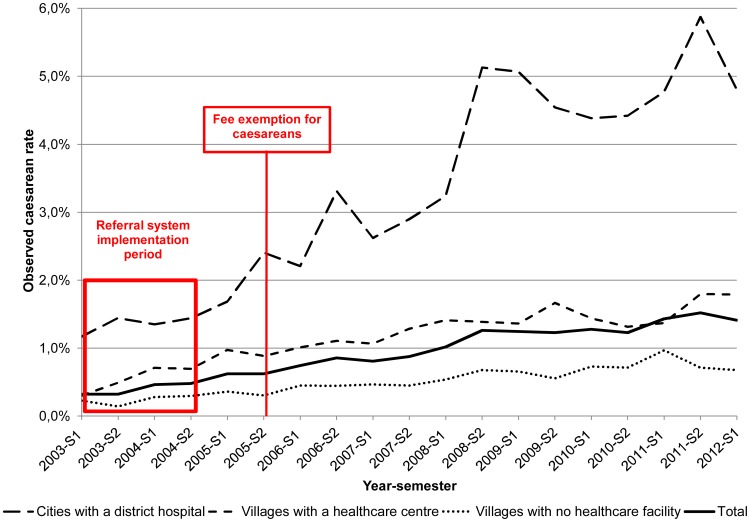
Methods: The observation period was from January 2003 to May 2012 in one Region and covered 11.7 million person-years. Exemption fees for caesareans were adopted on June 26, 2005. Data were obtained from a registration system implemented in 2003 that tracks all obstetrical emergencies and interventions including caesareans. The pre-intervention period was 30 months and the post-intervention period was 83 months. We used an interrupted time series to evaluate the trend before and after the policy adoption and the overall tendency.
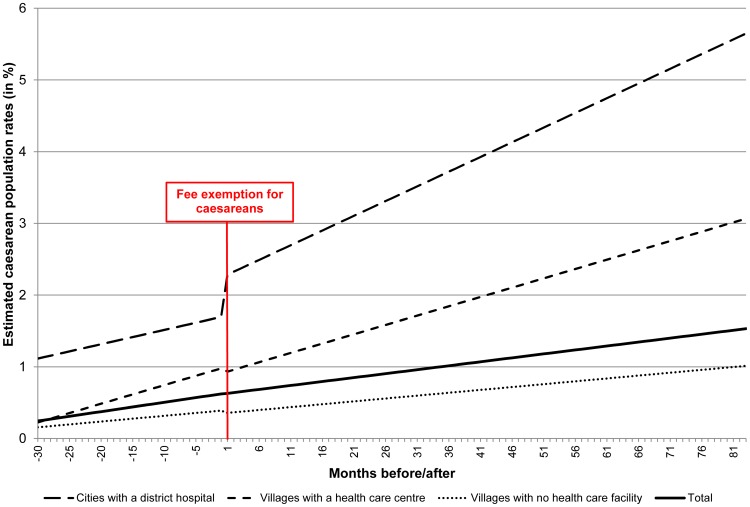
Findings: During the study period, the caesarean rate increased from 0.25 to 1.5% for the entire population. For women living in cities with district hospitals that provided caesareans, the rate increased from 1.7% before the policy was enforced to 5.7% 83 months later. No significant change in trends was observed among women living in villages with a healthcare centre or those in villages with no healthcare facility. For the latter, the caesarean rate increased from 0.4 to 1%.
Conclusions: After nine years of implementation policy in Mali, the caesarean rate achieved in cities with a district hospital reached the full beneficial effect of this measure, whereas for women living elsewhere this policy did not increase the caesarean rate to a level that could contribute effectively to reduce their risk of maternal death. Only universal access to this essential intervention could reduce the inequities and increase the effectiveness of this policy.
Conflict of interest statement
Figures
References
-
- Hogan MC, Foreman KJ, Naghavi M, Ahn SY, Wang M, et al. (2010) Maternal mortality for 181 countries, 1980–2008: a systematic analysis of progress towards Millennium Development Goal 5. Lancet 375: 1609–23. - PubMed
-
- Paxton A, Wardlaw T (2011) Are we making progress in maternal mortality? N Engl J Med 364: 1990–3. - PubMed
-
- Campbell OM, Graham WJ (2006) Strategies for reducing maternal mortality: getting on with what works. Lancet 368: 1284–99. - PubMed
-
- Ronsmans C, Graham WJ (2006) Maternal mortality: who, when, where, and why. Lancet 368: 1189–200. - PubMed
-
- Richard F, Ouedraogo C, De Brouwere V (2008) Quality cesarean delivery in Ouagadougou, Burkina Faso: a comprehensive approach. Int J Gynaecol Obstet 103: 283–90. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
