

Evaluation of the Dutch BRCA1/2 clinical genetic center referral criteria in an unselected early breast cancer population
- PMID: 25138101
- PMCID: PMC4402636
- DOI: 10.1038/ejhg.2014.161
Evaluation of the Dutch BRCA1/2 clinical genetic center referral criteria in an unselected early breast cancer population
Abstract
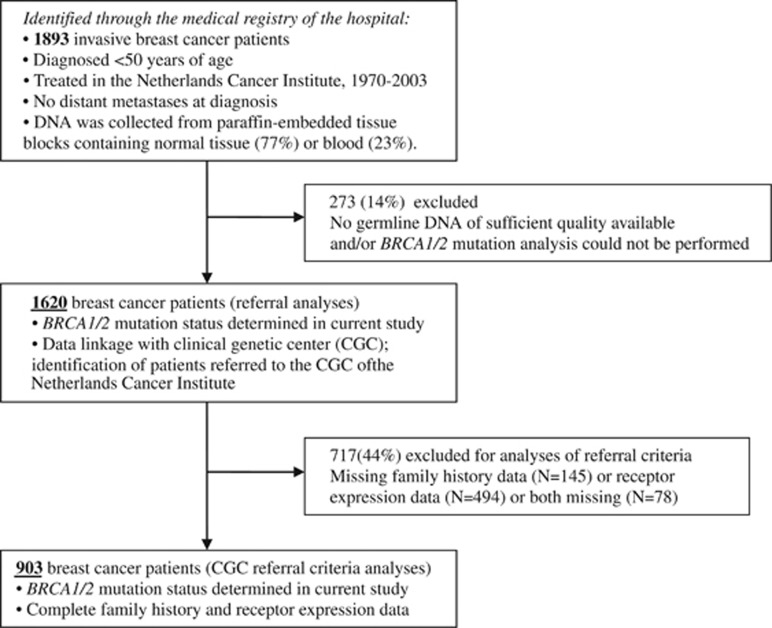
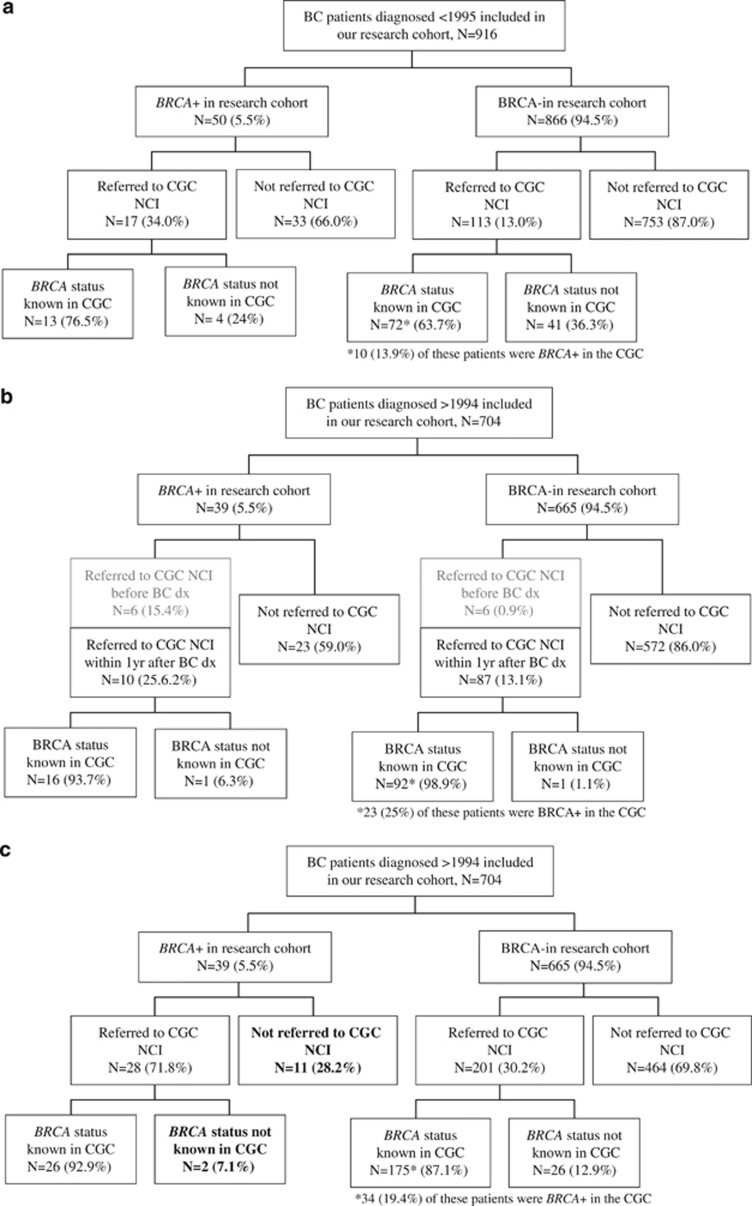
In this study, we evaluated the diagnostic value of the Dutch Clinical Genetic Center (CGC) referral guidelines for BRCA1/2 mutation testing in 903 early breast cancer patients, unselected for family history, diagnosed in a cancer hospital before the age of 50 years in 1974-2002; most prevalent Dutch pathogenic BRCA1/2 mutations had been analyzed on coded DNA in a research setting. Forty-nine (5.4%) of the patients were proven to be BRCA1/2 mutation carriers. We found that 78% and 69% of BRCA1 and BRCA2 mutation carriers identified met the criteria for referral to the CGC based on age, family history and synchronous multiple tumors; reflected by a combined sensitivity of 75.5% and specificity of 63.2%. More than half of the BRCA1 mutation carriers, that is, 58% had a triple-negative tumor. The highest AUC was obtained by shifting the age at diagnosis threshold criterion from 40 to 35 years and by adding a 'triple-negative breast cancer' criterion with an age threshold of 45 years; the specificity increased to 71.2%, whereas the sensitivity remained the same; that is, a referral of fewer patients will lead to the identification of at least the same number of BRCA1/2 mutation carriers. Two-thirds of the BRCA1/2 mutation carriers identified in this research setting had been referred for counseling and testing. Our results indicate that, awaiting a possibly more extended mutation screening of all breast cancer patients, the triple-negative status of a breast cancer should be added to the CGC referral criteria.
Figures
References
-
- Mavaddat N, Peock S, Frost D, et al. Cancer risks for BRCA1 and BRCA2 mutation carriers: results from prospective analysis of EMBRACE 4. J Natl Cancer Inst. 2013;105:812–822. - PubMed
-
- Brohet RM, Velthuizen ME, Hogervorst FB, et al. Breast and ovarian cancer risks in a large series of clinically ascertained families with a high proportion of BRCA1 and BRCA2 Dutch founder mutations 1. J Med Genet. 2014;51:98–107. - PubMed
-
- King MC, Marks JH, Mandell JB. Breast and ovarian cancer risks due to inherited mutations in BRCA1 and BRCA2. Science. 2003;302:643–646. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
