

Idiopathic normal pressure hydrocephalus: cerebral perfusion measured with pCASL before and repeatedly after CSF removal
- PMID: 25138210
- PMCID: PMC4269752
- DOI: 10.1038/jcbfm.2014.138
Idiopathic normal pressure hydrocephalus: cerebral perfusion measured with pCASL before and repeatedly after CSF removal
Abstract
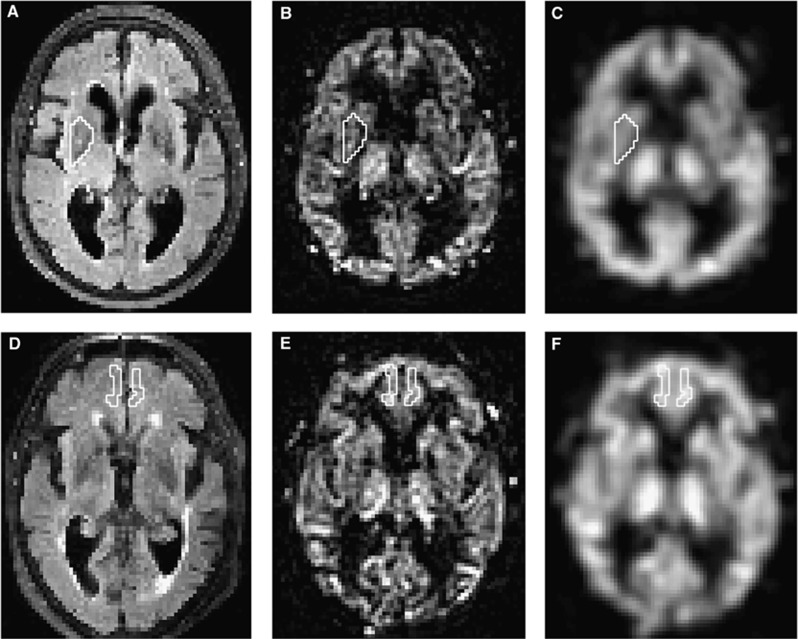
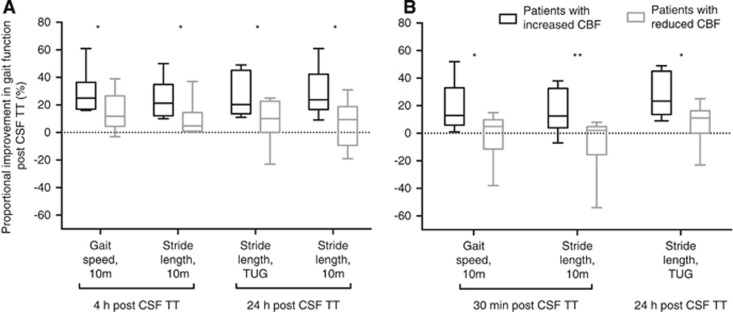
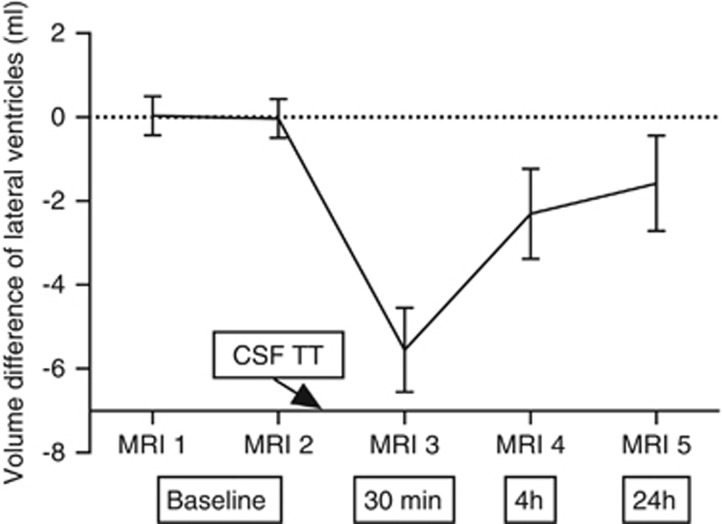
Pseudo-continuous arterial spin labeling (pCASL) measurements were performed in 20 patients with idiopathic normal pressure hydrocephalus (iNPH) to investigate whether cerebral blood flow (CBF) increases during the first 24 hours after a cerebrospinal fluid tap test (CSF TT). Five pCASL magnetic resonance imaging (MRI) scans were performed. Two scans were performed before removal of 40 mL CSF, and the other three at 30 minutes, 4 hours, and 24 hours, respectively after the CSF TT. Thirteen different regions of interest (ROIs) were manually drawn on coregistered MR images. In patients with increased CBF in lateral and frontal white matter after the CSF TT, gait function improved more than it did in patients with decreased CBF in these regions. However, in the whole sample, there was no significant increase in CBF after CSF removal compared with baseline investigations. The repeatability of CBF measurements at baseline was high, with intraclass correlation coefficients of 0.60 to 0.90 for different ROIs, but the median regional variability was in the range of 5% to 17%. Our results indicate that CBF in white matter close to the lateral ventricles plays a role in the reversibility of symptoms after CSF removal in patients with iNPH.
Figures
Similar articles
-
Arterial Spin-Labeling Perfusion MR Imaging Demonstrates Regional CBF Decrease in Idiopathic Normal Pressure Hydrocephalus.AJNR Am J Neuroradiol. 2017 Nov;38(11):2081-2088. doi: 10.3174/ajnr.A5347. Epub 2017 Aug 31. AJNR Am J Neuroradiol. 2017. PMID: 28860216 Free PMC article.
-
Cerebral Perfusion Does Not Increase after Shunt Surgery for Normal Pressure Hydrocephalus.J Neuroimaging. 2020 May;30(3):303-307. doi: 10.1111/jon.12702. Epub 2020 May 6. J Neuroimaging. 2020. PMID: 32374437
-
Pre-and postoperative cerebral blood flow changes in patients with idiopathic normal pressure hydrocephalus measured by computed tomography (CT)-perfusion.J Cereb Blood Flow Metab. 2016 Oct;36(10):1755-1766. doi: 10.1177/0271678X15608521. Epub 2015 Oct 14. J Cereb Blood Flow Metab. 2016. PMID: 26661191 Free PMC article.
-
Regional cerebral blood flow, white matter abnormalities, and cerebrospinal fluid hydrodynamics in patients with idiopathic adult hydrocephalus syndrome.J Neurol Neurosurg Psychiatry. 1996 Mar;60(3):282-8. doi: 10.1136/jnnp.60.3.282. J Neurol Neurosurg Psychiatry. 1996. PMID: 8609504 Free PMC article. Review.
-
Mathematical Modelling in Hydrocephalus.Neurol India. 2021 Nov-Dec;69(Supplement):S275-S282. doi: 10.4103/0028-3886.332259. Neurol India. 2021. PMID: 35102977 Review.
Cited by
-
Dynamic Susceptibility Contrast Perfusion Magnetic Resonance Imaging Demonstrates Reduced Periventricular Cerebral Blood Flow in Dogs with Ventriculomegaly.Front Vet Sci. 2017 Aug 22;4:137. doi: 10.3389/fvets.2017.00137. eCollection 2017. Front Vet Sci. 2017. PMID: 28879204 Free PMC article.
-
Association between the Onset of Idiopathic Normal Pressure Hydrocephalus Symptoms and Reduced Default Mode Network Connectivity.Dement Geriatr Cogn Disord. 2020;49(3):255-263. doi: 10.1159/000508338. Epub 2020 Aug 19. Dement Geriatr Cogn Disord. 2020. PMID: 32814322 Free PMC article.
-
Changes in postural stability after cerebrospinal fluid tap test in patients with idiopathic normal pressure hydrocephalus.Front Neurol. 2024 May 1;15:1361538. doi: 10.3389/fneur.2024.1361538. eCollection 2024. Front Neurol. 2024. PMID: 38751889 Free PMC article.
-
MRI assessment of the effects of acetazolamide and external lumbar drainage in idiopathic normal pressure hydrocephalus.Fluids Barriers CNS. 2015 Apr 2;12:9. doi: 10.1186/s12987-015-0004-z. Fluids Barriers CNS. 2015. PMID: 25928394 Free PMC article.
-
Aqueductal CSF Stroke Volume Is Increased in Patients with Idiopathic Normal Pressure Hydrocephalus and Decreases after Shunt Surgery.AJNR Am J Neuroradiol. 2019 Mar;40(3):453-459. doi: 10.3174/ajnr.A5972. Epub 2019 Feb 21. AJNR Am J Neuroradiol. 2019. PMID: 30792248 Free PMC article.
References
-
- Adams RD, Fisher CM, Hakim S, Ojemann RG, Sweet WH. Symptomatic occult hydrocephalus with ‘normal' cerebrospinal-fluid pressure—a treatable syndrome. N Engl J Med. 1965;273:117–126. - PubMed
-
- Owler BK, Pickard JD. Normal pressure hydrocephalus and cerebral blood flow: a review. Acta Neurol Scand. 2001;104:325–342. - PubMed
-
- Owler BK, Momjian S, Czosnyka Z, Czosnyka M, Pena A, Harris NG, et al. Normal pressure hydrocephalus and cerebral blood flow: a PET study of baseline values. J Cereb Blood Flow Metab. 2004;24:17–23. - PubMed
-
- Ziegelitz D, Starck G, Kristiansen D, Jakobsson M, Hultenmo M, Mikkelsen IK, et al. Cerebral perfusion measured by dynamic susceptibility contrast MRI is reduced in patients with idiopathic normal pressure hydrocephalus. J Magn Reson Imaging. 2013;39:1533–1542. - PubMed
-
- Relkin N, Marmarou A, Klinge P, Bergsneider M, Black PM. Diagnosing idiopathic normal-pressure hydrocephalus. Neurosurgery. 2005;57:S4–S16. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
