

The Lablite project: a cross-sectional mapping survey of decentralized HIV service provision in Malawi, Uganda and Zimbabwe
- PMID: 25138583
- PMCID: PMC4148932
- DOI: 10.1186/1472-6963-14-352
The Lablite project: a cross-sectional mapping survey of decentralized HIV service provision in Malawi, Uganda and Zimbabwe
Abstract
Background: In sub-Saharan Africa antiretroviral therapy (ART) is being decentralized from tertiary/secondary care facilities to primary care. The Lablite project supports effective decentralization in 3 countries. It began with a cross-sectional survey to describe HIV and ART services.
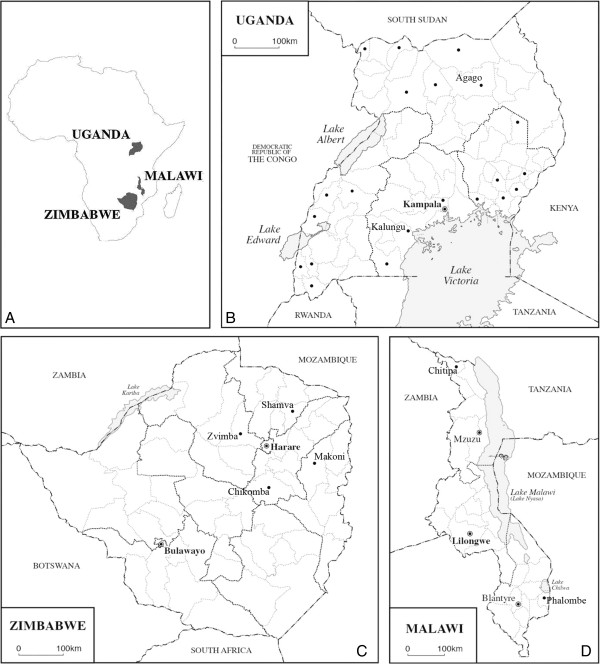
Methods: 81 purposively sampled health facilities in Malawi, Uganda and Zimbabwe were surveyed.
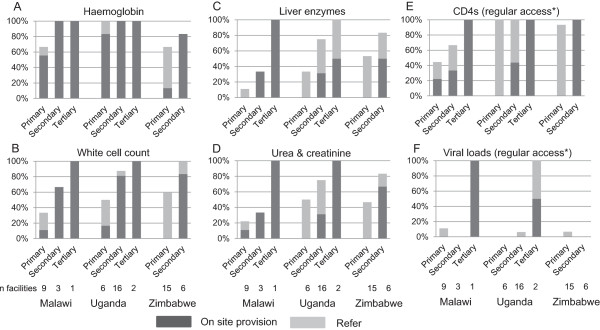
Results: The lowest level primary health centres comprised 16/20, 21/39 and 16/22 facilities included in Malawi, Uganda and Zimbabwe respectively. In Malawi and Uganda most primary health facilities had at least 1 medical assistant/clinical officer, with average 2.5 and 4 nurses/midwives for median catchment populations of 29,275 and 9,000 respectively. Primary health facilities in Zimbabwe were run by nurses/midwives, with average 6 for a median catchment population of 8,616. All primary health facilities provided HIV testing and counselling, 50/53 (94%) cotrimoxazole preventive therapy (CPT), 52/53 (98%) prevention of mother-to-child transmission of HIV (PMTCT) and 30/53 (57%) ART management (1/30 post ART-initiation follow-up only). All secondary and tertiary-level facilities provided HIV and ART services. In total, 58/81 had ART provision. Stock-outs during the 3 months prior to survey occurred across facility levels for HIV test-kits in 55%, 26% and 9% facilities in Malawi, Uganda and Zimbabwe respectively; for CPT in 58%, 32% and 9% and for PMTCT drugs in 26%, 10% and 0% of facilities (excluding facilities where patients were referred out for either drug). Across all countries, in facilities with ART stored on-site, adult ART stock-outs were reported in 3/44 (7%) facilities compared with 10/43 (23%) facility stock-outs of paediatric ART. Laboratory services at primary health facilities were limited: CD4 was used for ART initiation in 4/9, 5/6 and 13/14 in Malawi, Uganda and Zimbabwe respectively, but frequently only in selected patients. Routine viral load monitoring was not used; 6/58 (10%) facilities with ART provision accessed centralised viral loads for selected patients.
Conclusions: Although coverage of HIV testing, PMTCT and cotrimoxazole prophylaxis was high in all countries, decentralization of ART services was variable and incomplete. Challenges of staffing and stock management were evident. Laboratory testing for toxicity and treatment effectiveness monitoring was not available in most primary level facilities.
Figures
References
-
- National Drug and Therapeutics Policy Advisory Committee and The AIDS and TB Unit, Zimbabwe Ministry of Health and Child Welfare . Guidelines for Antiretroviral Therapy in Zimbabwe. Harare: Government of Zimbabwe; 2010.
-
- Katabira ET, Kamya MR, Kalyesubula I, Namale A, Uganda Ministry of Health . STD/AIDS Control Programme, Ministry of Health Uganda. 3. Kampala: Ministry of Health Uganda; 2009. National Antiretroviral Treatment Guidelines for Adults, Adolescents and Children.
-
- Department of HIV and AIDS, Malawi Ministry of Health . Clinical Management of HIV in Children and Adults. 1. Lilongwe: Malawi Ministry of Health; 2011.
-
- Bemelmans M, van den Akker T, Ford N, Philips M, Zachariah R, Harries A, Schouten E, Hermann K, Mwagomba B, Massaquoi M. Providing universal access to antiretroviral therapy in Thyolo, Malawi through task shifting and decentralization of HIV/AIDS care. Trop Med Int Health. 2010;15(12):1413–1420. doi: 10.1111/j.1365-3156.2010.02649.x. - DOI - PubMed
Pre-publication history
-
- The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1472-6963/14/352/prepub
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
