

Third-wave cognitive therapy versus mentalisation-based treatment for major depressive disorder: a randomised clinical trial
- PMID: 25138802
- PMCID: PMC4139625
- DOI: 10.1136/bmjopen-2014-004903
Third-wave cognitive therapy versus mentalisation-based treatment for major depressive disorder: a randomised clinical trial
Abstract
Objective: To compare the benefits and harms of third-wave cognitive therapy versus mentalisation-based therapy in a small sample of depressed participants.
Setting: The trial was conducted at an outpatient psychiatric clinic for non-psychotic patients in Roskilde, Denmark.
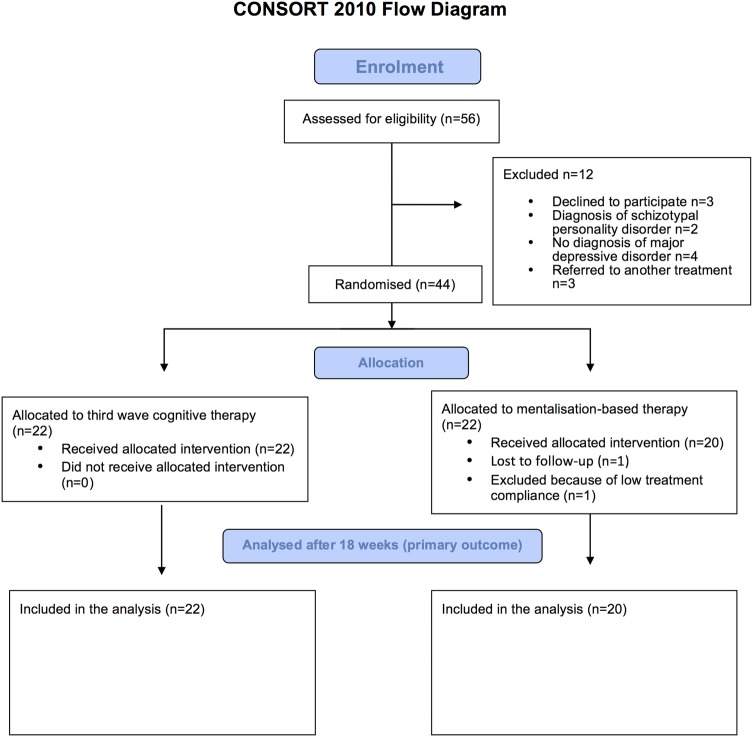
Participants: 44 consecutive adult participants diagnosed with major depressive disorder.
Interventions: 18 weeks of third-wave cognitive therapy (n=22) versus 18 weeks of mentalisation-based treatment (n=22).
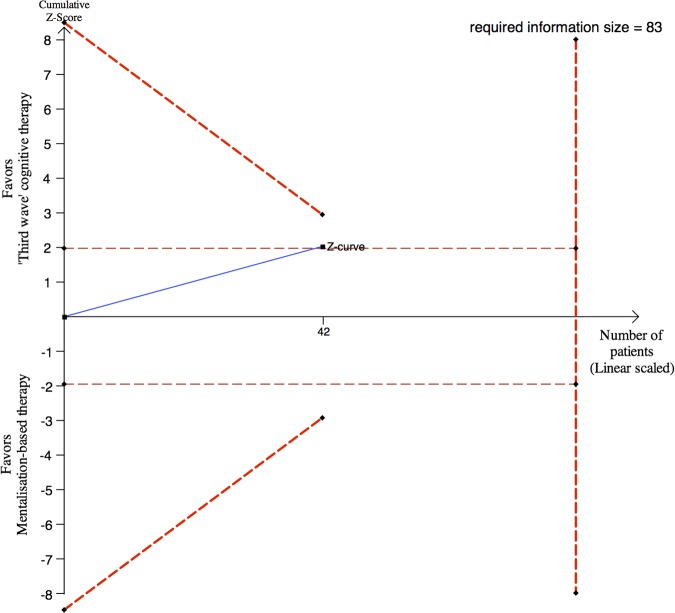
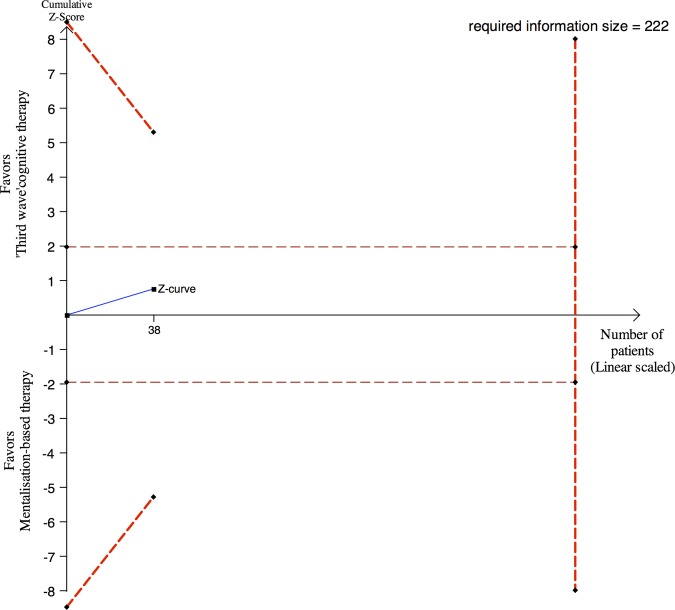
Outcomes: The primary outcome was the Hamilton Rating Scale for Depression (HDRS) at end of treatment (18 weeks). Secondary outcomes were: remission (HDRS <8), Beck's Depression Inventory, Symptom Checklist 90 Revised and The WHO-Five Well-being Index 1999.
Results: The trial inclusion lasted for about 2 years as planned but only 44 out of the planned 84 participants were randomised. Two mentalisation-based participants were lost to follow-up. The unadjusted analysis showed that third-wave participants compared with mentalisation-based participants did not differ significantly regarding the 18 weeks HDRS score (12.9 vs 17.0; mean difference -4.14; 95% CI -8.30 to 0.03; p=0.051). In the analysis adjusted for baseline HDRS score, the difference was favouring third-wave cognitive therapy (p=0.039). At 18 weeks, five of the third-wave participants (22.7%) were in remission versus none of the mentalisation-based participants (p=0.049). We recorded no suicide attempts or suicides during the intervention period in any of the 44 participants. No significant differences were found between the two intervention groups on the remaining secondary outcomes.
Conclusions: Third-wave cognitive therapy may be more effective than mentalisation-based therapy for depressive symptoms measured on the HDRS. However, more randomised clinical trials are needed to assess the effects of third-wave cognitive therapy and mentalisation-based treatment for depression.
Trial registration number: Registered with Clinical Trials government identifier: NCT01070134.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
References
-
- Kahl KG, Winter L, Schweiger U, et al. The third wave of cognitive-behavioural psychotherapies: concepts and efficacy. Fortschr Neurol Psychiatr 2011;79:330–9 - PubMed
-
- Linehan MM, Comtois KA, Murray AM, et al. Two year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviours an borderline personality disorder. Arch Gen Psychiatry 2006;63:757–66 - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical