

Use of clarithromycin and roxithromycin and risk of cardiac death: cohort study
- PMID: 25139799
- PMCID: PMC4138354
- DOI: 10.1136/bmj.g4930
Use of clarithromycin and roxithromycin and risk of cardiac death: cohort study
Abstract
Objective: To assess the risk of cardiac death associated with the use of clarithromycin and roxithromycin.
Design: Cohort study.
Setting: Denmark, 1997-2011.
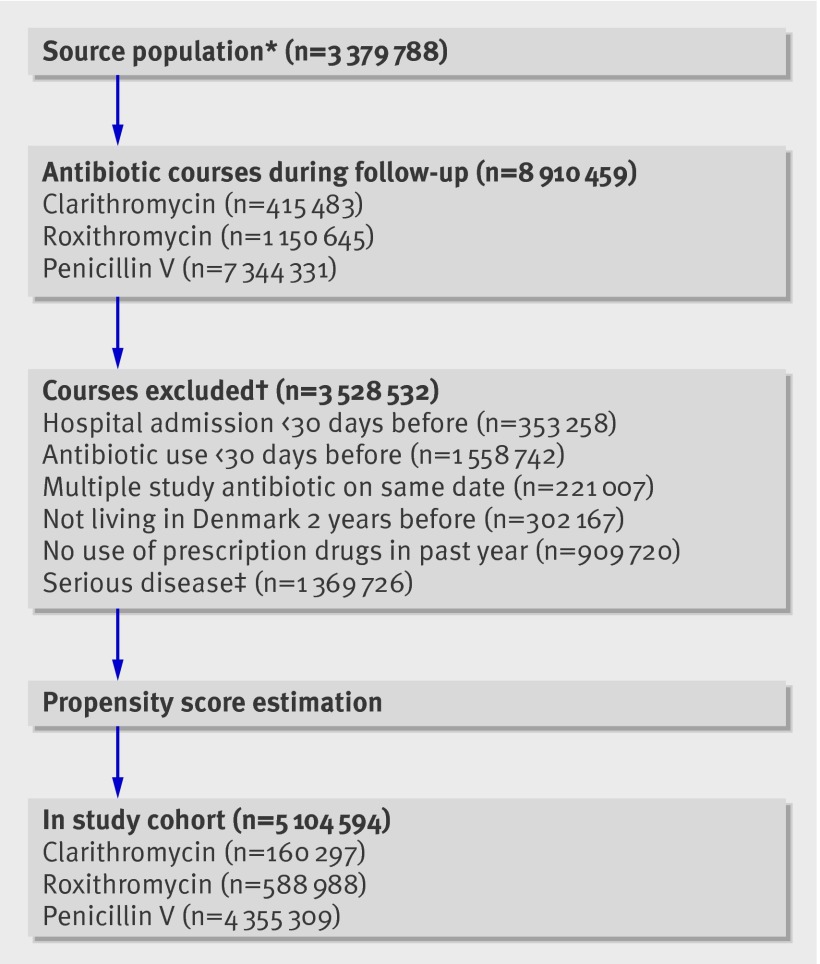
Participants: Danish adults, 40-74 years of age, who received seven day treatment courses with clarithromycin (n = 160,297), roxithromycin (n = 588,988), and penicillin V (n = 4,355,309).
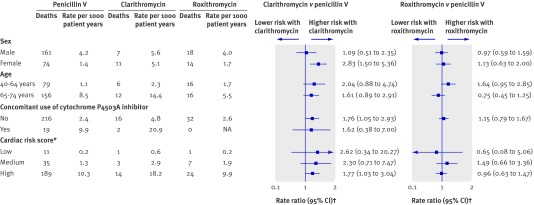
Main outcome measures: The main outcome was risk of cardiac death associated with clarithromycin and roxithromycin, compared with penicillin V. Subgroup analyses were conducted according to sex, age, risk score, and concomitant use of drugs that inhibit the cytochrome P450 3A enzyme, which metabolises macrolides.
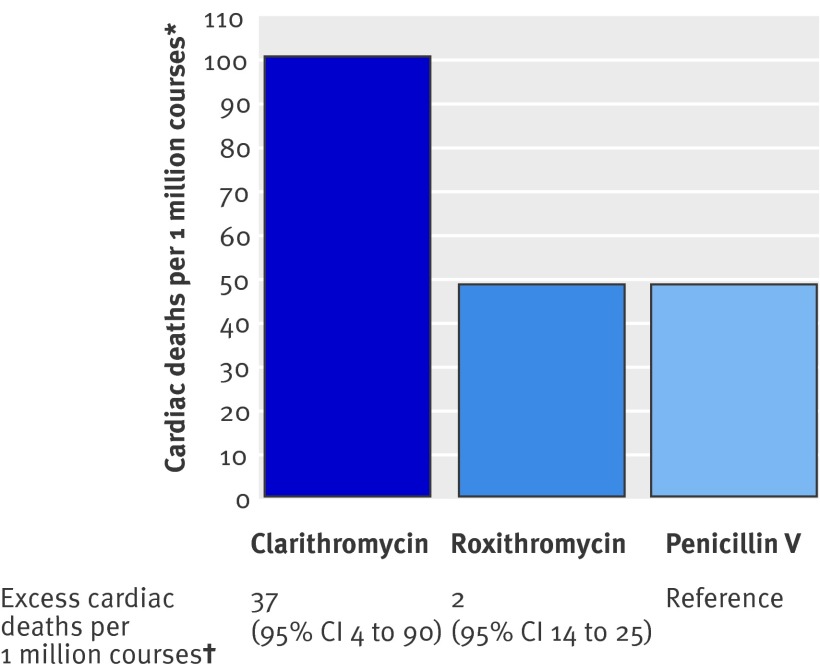
Results: A total of 285 cardiac deaths were observed. Compared with use of penicillin V (incidence rate 2.5 per 1000 person years), use of clarithromycin was associated with a significantly increased risk of cardiac death (5.3 per 1000 person years; adjusted rate ratio 1.76, 95% confidence interval 1.08 to 2.85) but use of roxithromycin was not (2.5 per 1000 person years; adjusted rate ratio 1.04, 0.72 to 1.51). The association with clarithromycin was most pronounced among women (adjusted rate ratios 2.83 (1.50 to 5.36) in women and 1.09 (0.51 to 2.35) in men). Compared with penicillin V, the adjusted absolute risk difference was 37 (95% confidence interval 4 to 90) cardiac deaths per 1 million courses with clarithromycin and 2 (-14 to 25) cardiac deaths per 1 million courses with roxithromycin.
Conclusions: This large cohort study found a significantly increased risk of cardiac death associated with clarithromycin. No increased risk was seen with roxithromycin. Given the widespread use of clarithromycin, these findings call for confirmation in independent populations.
© Svanström et al 2014.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- Justo D, Zeltser D. Torsades de pointes induced by antibiotics. Eur J Intern Med 2006;17:254-9. - PubMed
-
- Mosholder AD, Mathew J, Alexander JJ, Smith H, Nambiar S. Cardiovascular risks with azithromycin and other antibacterial drugs. N Engl J Med 2013;368:1665-8. - PubMed
-
- Owens RC Jr, Nolin TD. Antimicrobial-associated QT interval prolongation: pointes of interest. Clin Infect Dis 2006;43:1603-11. - PubMed
-
- Hensey C, Keane D. Clarithromycin induced torsade de pointes. Ir J Med Sci 2008;177:67-8. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous