

End-stage renal disease and survival in people with diabetes: a national database linkage study
- PMID: 25140030
- PMCID: PMC4309927
- DOI: 10.1093/qjmed/hcu170
End-stage renal disease and survival in people with diabetes: a national database linkage study
Abstract
Background: Increasing prevalence of diabetes worldwide is projected to lead to an increase in patients with end-stage renal disease (ESRD) requiring renal replacement therapy (RRT).
Aim: To provide contemporary estimates of the prevalence of ESRD and requirement for RRT among people with diabetes in a nationwide study and to report associated survival.
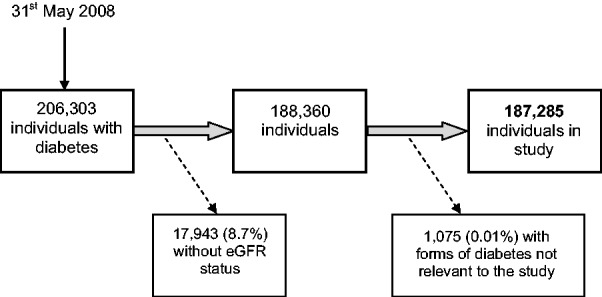
Methods: Data were extracted and linked from three national databases: Scottish Renal Registry, Scottish Care Initiative-Diabetes Collaboration and National Records of Scotland death data. Survival analyses were modelled with Cox regression.
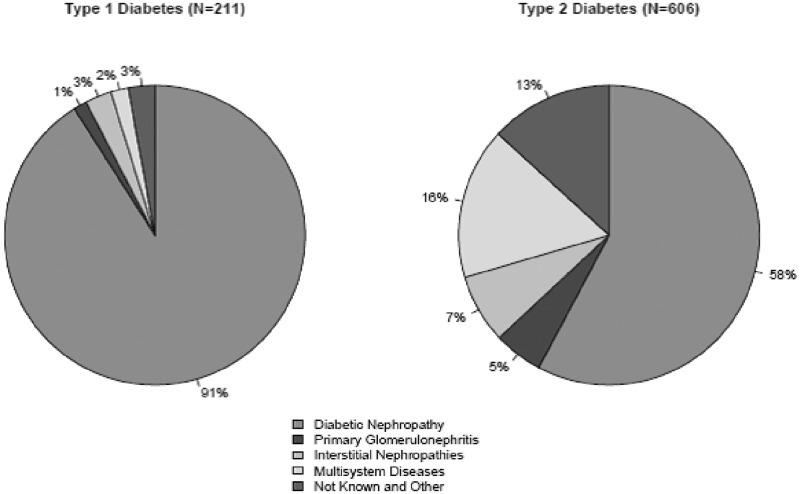
Results: Point prevalence of chronic kidney disease (CKD)5 in 2008 was 1.63% of 19 414 people with type 1 diabetes (T1DM) compared with 0.58% of 167 871 people with type 2 diabetes (T2DM) (odds ratio for DM type 0.97, P = 0.77, on adjustment for duration. Although 83% of those with T1DM and CKD5 and 61% of those with T2DM and CKD5 were receiving RRT, there was no difference when adjusted for age, sex and DM duration (odds ratio for DM type 0.83, P = 0.432). Diabetic nephropathy was the primary renal diagnosis in 91% of people with T1DM and 58% of people with T2DM on RRT. Median survival time from initiation of RRT was 3.84 years (95% CI 2.77, 4.62) in T1DM and 2.16 years (95% CI: 1.92, 2.38) in T2DM.
Conclusion: Considerable numbers of patients with diabetes continue to progress to CKD5 and RRT. Almost half of all RRT cases in T2DM are considered to be due to conditions other than diabetic nephropathy. Median survival time for people with diabetes from initiation of RRT remains poor. These prevalence data are important for future resource planning.
© The Author 2014. Published by Oxford University Press on behalf of the Association of Physicians.
Figures
References
-
- International Diabetes Federation. IDF Diabetes Atlas. 6th edn. Brussels, Belgium: International Diabetes Federation; 2013. . http://www.idf.org/diabetesatlas (18 April 2014, date last accessed) - PubMed
-
- Scottish Diabetes Survey Monitoring Group. Scottish Diabetes Survey 2003. Scotland: NHS National Services; www.scotland.gov.uk/Publications/2004/10/20023/44194 (19 April 2014, date last accessed)
-
- Scottish Diabetes Survey Monitoring Group. Scottish Diabetes Survey 2012. Scotland: NHS National Services; www.diabetesinscotland.org/Publications/SDS%202012.pdf(19 April 2014, date last accessed)
-
- Van Dijk PC, Jager KJ, Stengel B, Gronhagen-Riska C, Feest TG, Briggs JD. Renal replacement therapy for diabetic end-stage renal disease: data from 10 registries in Europe (1991–2000) Kidney Int. 2005;67:1489–99. - PubMed
-
- Information Services Division NHS National Services Scotland. Scottish Renal Registry report 2011. NHS National Services Scotland 2012.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
