

Oligonucleotide ligation assay detects HIV drug resistance associated with virologic failure among antiretroviral-naive adults in Kenya
- PMID: 25140907
- PMCID: PMC4197120
- DOI: 10.1097/QAI.0000000000000312
Oligonucleotide ligation assay detects HIV drug resistance associated with virologic failure among antiretroviral-naive adults in Kenya
Abstract
Background: Transmitted drug resistance (TDR) is increasing in some areas of Africa. Detection of TDR may predict virologic failure of first-line nonnucleoside reverse transcriptase inhibitor (NNRTI)-based antiretroviral therapy (ART). We evaluated the utility of a relatively inexpensive oligonucleotide ligation assay (OLA) to detect clinically relevant TDR at the time of ART initiation.
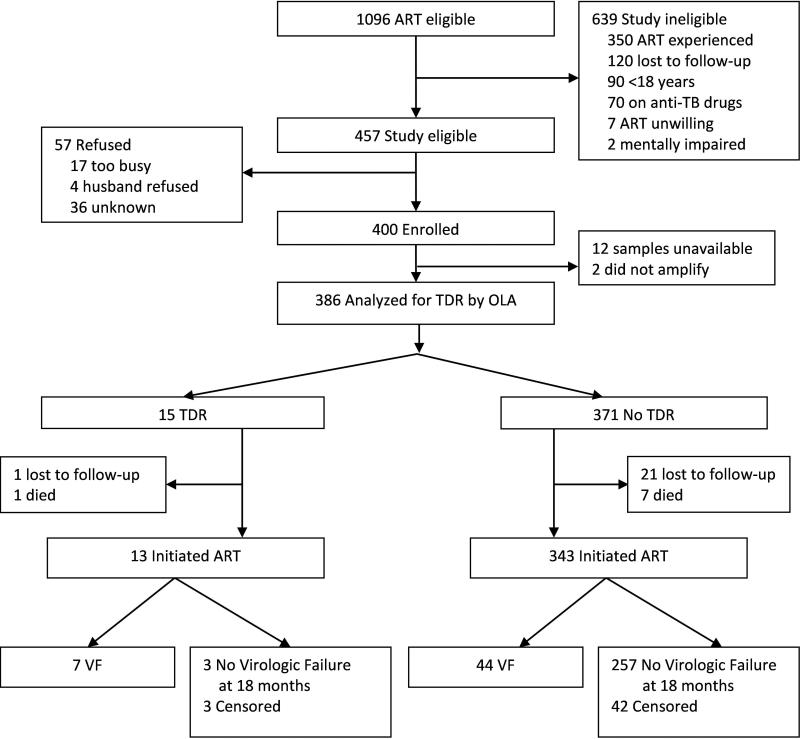
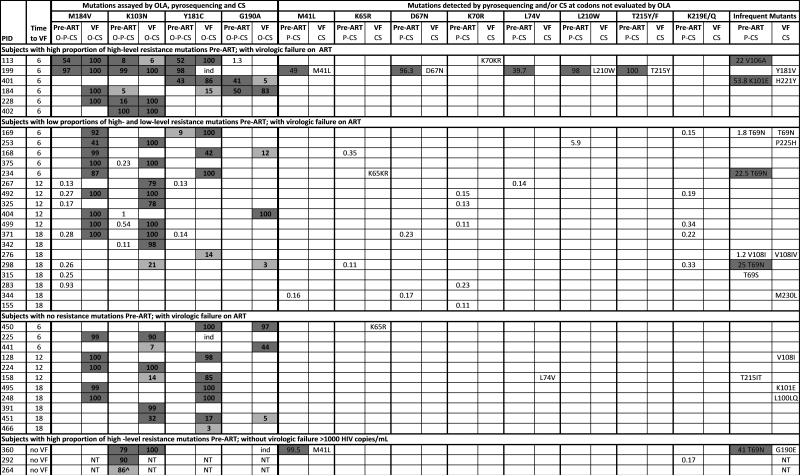
Methods: Pre-ART plasmas from ART-naive Kenyans initiating an NNRTI-based fixed-dose combination ART in a randomized adherence trial conducted in 2006 were retrospectively analyzed by OLA for mutations conferring resistance to NNRTI (K103N, Y181C, and G190A) and lamivudine (M184V). Post-ART plasmas were analyzed for virologic failure (≥1000 copies/mL) at 6-month intervals over 18-month follow-up. Pre-ART plasmas of those with virologic failure were evaluated for drug resistance by consensus and 454-pyrosequencing.
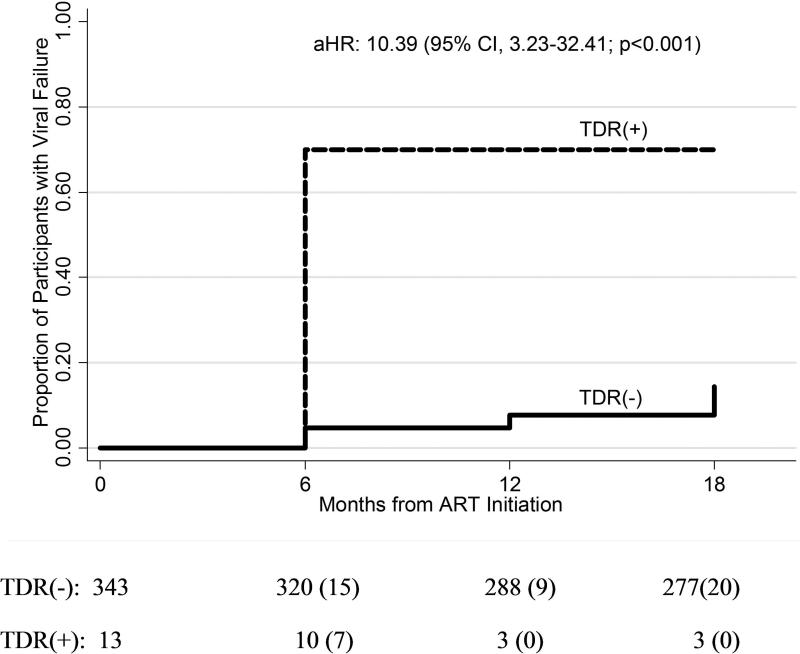
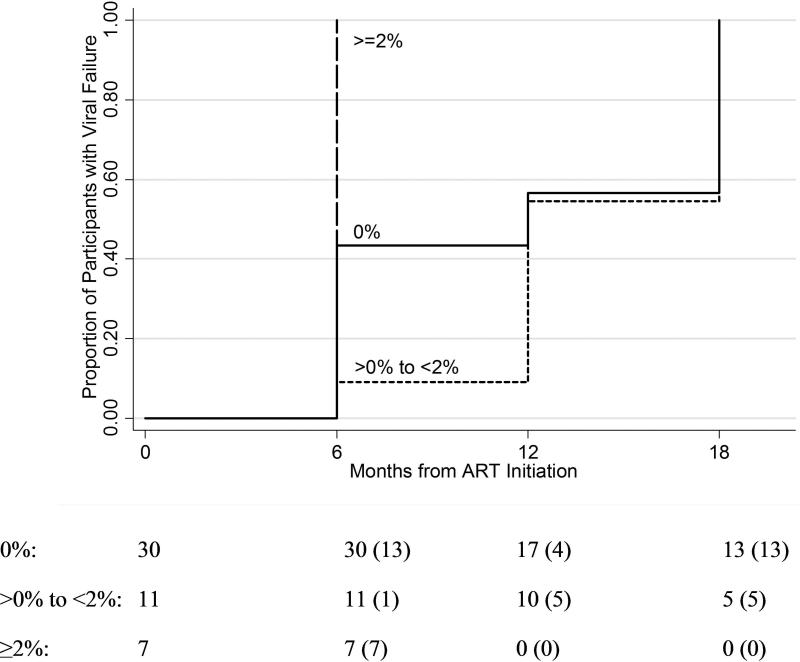
Results: Among 386 participants, TDR was detected by OLA in 3.89% (95% confidence interval: 2.19 to 6.33) and was associated with a 10-fold higher rate of virologic failure (hazard ratio: 10.39; 95% confidence interval: 3.23 to 32.41; P < 0.001) compared with those without TDR. OLA detected 24 TDR mutations (K103N: n = 13; Y181C: n = 5; G190A: n = 3; M184V: n = 3) in 15 subjects (NNRTI: n = 15; 3TC: n = 3). Among 51 participants who developed virologic failure, consensus sequencing did not detect additional TDR mutations conferring high-level resistance, and pyrosequencing only detected additional mutations at frequencies <2%. Mutant frequencies <2% at ART initiation were significantly less likely to be found at the time of virologic failure compared with frequencies ≥2% (22% vs. 63%; P < 0.001).
Conclusions: Detection of TDR by a point mutation assay may prevent the use of suboptimal ART.
Figures
References
-
- UNAIDS . Global report: UNAIDS report on the global AIDS epidemic 2012. UNAIDS; Geneva: 2012.
-
- Gupta RK, Jordan MR, Sultan BJ, et al. Global trends in antiretroviral resistance in treatment-naive individuals with HIV after rollout of antiretroviral treatment in resource-limited settings: a global collaborative study and meta-regression analysis. Lancet. 2012 Oct 6;380(9849):1250–1258. - PMC - PubMed
-
- Barth RE, Wensing AM, Tempelman HA, Moraba R, Schuurman R, Hoepelman AI. Rapid accumulation of nonnucleoside reverse transcriptase inhibitor-associated resistance: evidence of transmitted resistance in rural South Africa. AIDS. 2008 Oct 18;22(16):2210–2212. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
