

Effect of cognitive therapy with antidepressant medications vs antidepressants alone on the rate of recovery in major depressive disorder: a randomized clinical trial
- PMID: 25142196
- PMCID: PMC4315327
- DOI: 10.1001/jamapsychiatry.2014.1054
Effect of cognitive therapy with antidepressant medications vs antidepressants alone on the rate of recovery in major depressive disorder: a randomized clinical trial
Retraction in
-
Notice of Retraction and Replacement. Hollon et al. Effect of cognitive therapy with antidepressant medications vs antidepressants alone on the rate of recovery in major depressive disorder: a randomized clinical trial. JAMA Psychiatry. 2014;71(10):1157-1164.JAMA Psychiatry. 2016 Jun 1;73(6):639-40. doi: 10.1001/jamapsychiatry.2016.0756. JAMA Psychiatry. 2016. PMID: 27097060 Free PMC article. No abstract available.
Abstract
Importance: Antidepressant medication (ADM) is efficacious in the treatment of depression, but not all patients achieve remission and fewer still achieve recovery with ADM alone.
Objective: To determine the effects of combining cognitive therapy (CT) with ADM vs ADM alone on remission and recovery in major depressive disorder (MDD).
Design, setting, and participants: A total of 452 adult outpatients with chronic or recurrent MDD participated in a trial conducted in research clinics at 3 university medical centers in the United States. The patients were randomly assigned to ADM treatment alone or CT combined with ADM treatment. Treatment was continued for up to 42 months until recovery was achieved.
Interventions: Antidepressant medication with or without CT.
Main outcomes and measures: Blind evaluations of recovery with a modified version of the 17-item Hamilton Rating Scale for Depression and the Longitudinal Interval Follow-up Evaluation.
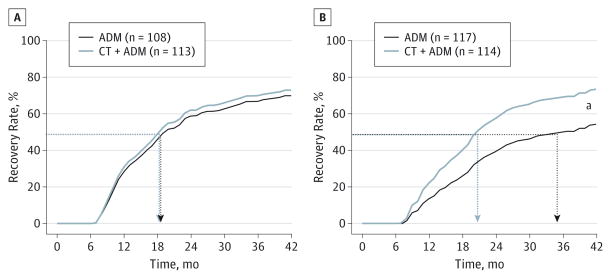
Results: Combined treatment enhanced the rate of recovery vs treatment with ADM alone (72.6% vs 62.5%; t451 = 2.45; P = .01; hazard ratio [HR], 1.33; 95% CI, 1.06-1.68; number needed to treat [NNT], 10; 95% CI, 5-72). This effect was conditioned on interactions with severity (t451 = 1.97; P = .05; NNT, 5) and chronicity (χ2 = 7.46; P = .02; NNT, 6) such that the advantage for combined treatment was limited to patients with severe, nonchronic MDD (81.3% vs 51.7%; n = 146; t145 = 3.96; P = .001; HR, 2.34; 95% CI, 1.54-3.57; NNT, 3; 95% CI, 2-5). Fewer patients dropped out of combined treatment vs ADM treatment alone (18.9% vs 26.8%; t451 = -2.04; P = .04; HR, 0.66; 95% CI, 0.45-0.98). Remission rates did not differ significantly either as a main effect of treatment or as an interaction with severity or chronicity. Patients with comorbid Axis II disorders took longer to recover than did patients without comorbid Axis II disorders regardless of the condition (P = .01). Patients who received combined treatment reported fewer serious adverse events than did patients who received ADMs alone (49 vs 71; P = .02), largely because they experienced less time in an MDD episode.
Conclusions and relevance: Cognitive therapy combined with ADM treatment enhances the rates of recovery from MDD relative to ADMs alone, with the effect limited to patients with severe, nonchronic depression.
Trial registration: clinicaltrials.gov Identifier: NCT00057577.
Conflict of interest statement
Figures


Comment in
-
Large-scale study suggests specific indicators for combined cognitive therapy and pharmacotherapy in major depressive disorder.JAMA Psychiatry. 2014 Oct;71(10):1101-2. doi: 10.1001/jamapsychiatry.2014.1524. JAMA Psychiatry. 2014. PMID: 25142013 No abstract available.
-
Cognitive therapy plus medication management is better than antidepressants alone for patients with severe depression.Evid Based Ment Health. 2015 Aug;18(3):95. doi: 10.1136/eb-2014-102012. Epub 2015 Jun 24. Evid Based Ment Health. 2015. PMID: 26109592 Free PMC article. No abstract available.
References
-
- Keller MB. Past, present, and future directions for defining optimal treatment outcome in depression: remission and beyond. JAMA. 2003;289(23):3152–3160. - PubMed
-
- Rush AJ, Kraemer HC, Sackeim HA, et al. ACNP Task Force. Report by the ACNP Task Force on response and remission in major depressive disorder. Neuropsychopharmacology. 2006;31(9):1841–1853. - PubMed
-
- Marcus SC, Olfson M. National trends in the treatment for depression from 1998 to 2007. Arch Gen Psychiatry. 2010;67(12):1265–1273. - PubMed
-
- Psychiatry Online. Practice guideline for the treatment of patients with major depressive disorder: 3rd rev. Washington, DC: American Psychiatric Association; 2010. [Accessed October 9, 2012]. American Psychiatric Association Practice Guidelines. http:www.psychiatryonline.com/pracGuide/pracGuideTopic_7.aspx.
-
- Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am J Psychiatry. 2006;163 (11):1905–1917. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
