

Chronic passive venous congestion drives hepatic fibrogenesis via sinusoidal thrombosis and mechanical forces
- PMID: 25142214
- PMCID: PMC4303520
- DOI: 10.1002/hep.27387
Chronic passive venous congestion drives hepatic fibrogenesis via sinusoidal thrombosis and mechanical forces
Abstract
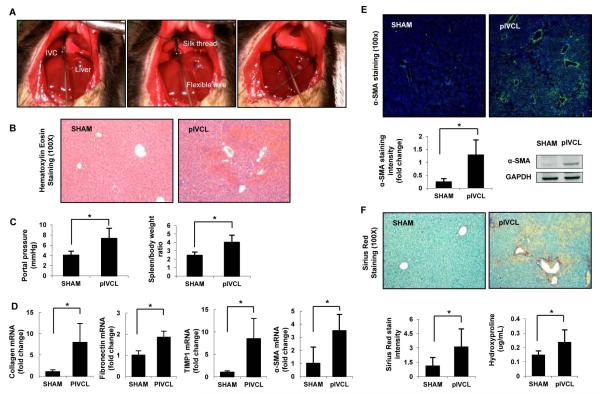
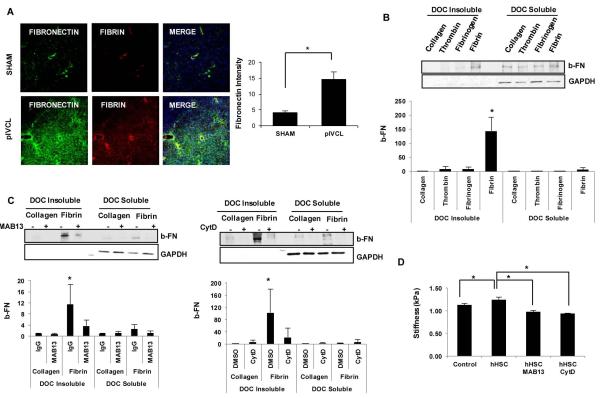
Chronic passive hepatic congestion (congestive hepatopathy) leads to hepatic fibrosis; however, the mechanisms involved in this process are not well understood. We developed a murine experimental model of congestive hepatopathy through partial ligation of the inferior vena cava (pIVCL). C57BL/6 and transgenic mice overexpressing tissue factor pathway inhibitor (SM22α-TFPI) were subjected to pIVCL or sham. Liver and blood samples were collected and analyzed in immunohistochemical, morphometric, real-time polymerase chain reaction, and western blot assays. Hepatic fibrosis and portal pressure were significantly increased after pIVCL concurrent with hepatic stellate cell (HSC) activation. Liver stiffness, as assessed by magnetic resonance elastography, correlated with portal pressure and preceded fibrosis in our model. Hepatic sinusoidal thrombosis as evidenced by fibrin deposition was demonstrated both in mice after pIVCL as well as in humans with congestive hepatopathy. Warfarin treatment and TFPI overexpression both had a protective effect on fibrosis development and HSC activation after pIVCL. In vitro studies show that congestion stimulates HSC fibronectin (FN) fibril assembly through direct effects of thrombi as well as by virtue of mechanical strain. Pretreatment with either Mab13 or Cytochalasin-D, to inhibit β-integrin or actin polymerization, respectively, significantly reduced fibrin and stretch-induced FN fibril assembly.
Conclusion: Chronic hepatic congestion leads to sinusoidal thrombosis and strain, which in turn promote hepatic fibrosis. These studies mechanistically link congestive hepatopathy to hepatic fibrosis.
© 2014 by the American Association for the Study of Liver Diseases.
Figures






Comment in
-
Hepatic congestion leads to fibrosis: findings in a newly developed murine model.Hepatology. 2015 Feb;61(2):428-30. doi: 10.1002/hep.27550. Epub 2015 Jan 5. Hepatology. 2015. PMID: 25283276 Free PMC article. No abstract available.
References
-
- Ahmed A. American College of Cardiology/American Heart Association Chronic Heart Failure Evaluation and Management guidelines: relevance to the geriatric practice. Journal of the American Geriatrics Society. 2003;51:123–126. - PubMed
-
- de Leval MR, Deanfield JE. Four decades of Fontan palliation. Nature reviews. Cardiology. 2010;7:520–527. - PubMed
-
- Asrani SK, Asrani NS, Freese DK, Phillips SD, Warnes CA, Heimbach J, Kamath PS. Congenital heart disease and the liver. Hepatology. 2012;56:1160–1169. - PubMed
-
- Wanless IR, Liu JJ, Butany J. Role of thrombosis in the pathogenesis of congestive hepatic fibrosis (cardiac cirrhosis) Hepatology. 1995;21:1232–1237. - PubMed
-
- Wanless IR, Wong F, Blendis LM, Greig P, Heathcote EJ, Levy G. Hepatic and portal vein thrombosis in cirrhosis: possible role in development of parenchymal extinction and portal hypertension. Hepatology. 1995;21:1238–1247. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous