

Triage: care of the critically ill and injured during pandemics and disasters: CHEST consensus statement
- PMID: 25144591
- PMCID: PMC7127536
- DOI: 10.1378/chest.14-0736
Triage: care of the critically ill and injured during pandemics and disasters: CHEST consensus statement
Abstract
Background: Pandemics and disasters can result in large numbers of critically ill or injured patients who may overwhelm available resources despite implementing surge-response strategies. If this occurs, critical care triage, which includes both prioritizing patients for care and rationing scarce resources, will be required. The suggestions in this chapter are important for all who are involved in large-scale pandemics or disasters with multiple critically ill or injured patients, including front-line clinicians, hospital administrators, and public health or government officials.
Methods: The Triage topic panel reviewed previous task force suggestions and the literature to identify 17 key questions for which specific literature searches were then conducted to identify studies upon which evidence-based recommendations could be made. No studies of sufficient quality were identified. Therefore, the panel developed expert opinion-based suggestions using a modified Delphi process. Suggestions from the previous task force that were not being updated were also included for validation by the expert panel.
Results: The suggestions from the task force outline the key principles upon which critical care triage should be based as well as a path for the development of the plans, processes, and infrastructure required. This article provides 11 suggestions regarding the principles upon which critical care triage should be based and policies to guide critical care triage.
Conclusions: Ethical and efficient critical care triage is a complex process that requires significant planning and preparation. At present, the prognostic tools required to produce an effective decision support system (triage protocol) as well as the infrastructure, processes, legal protections, and training are largely lacking in most jurisdictions. Therefore, critical care triage should be a last resort after mass critical care surge strategies.
Figures
References
-
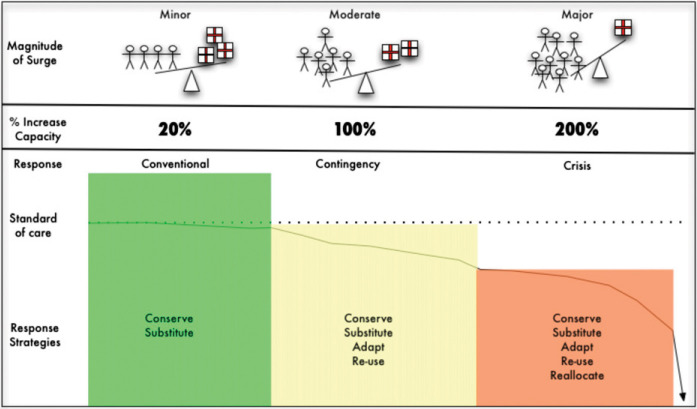
- Hick JL, Barbera JA, Kelen GD. Refining surge capacity: conventional, contingency, and crisis capacity. Disaster Med Public Health Prep. 2009;3(suppl 1):S59–S67. - PubMed
-
- Hick JL, Christian MD, Sprung CL. European Society of Intensive Care Medicine's Task Force for Intensive Care Unit Triage During an Influenza Epidemic or Mass Disaster. Chapter 2. Surge capacity and infrastructure considerations for mass critical care. Recommendations and standard operating procedures for intensive care unit and hospital preparations for an influenza epidemic or mass disaster. Intensive Care Med. 2010;36(suppl 1):S11–S20. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
