

Clinical outcome in acute small bowel obstruction after surgical or conservative management
- PMID: 25145820
- PMCID: PMC4232739
- DOI: 10.1007/s00268-014-2733-6
Clinical outcome in acute small bowel obstruction after surgical or conservative management
Abstract
Background: Small bowel obstruction (SBO) is characterized by a high rate of recurrence. In the present study, we aimed to compare the outcomes of patients managed either by conservative treatment or surgical operation for an episode of SBO.
Methods: The outcomes of all patients hospitalized at a single center for acute SBO between 2004 and 2007 were assessed. The occurrence of recurrent hospitalization, surgery, SBO symptoms at home, and mortality was determined.
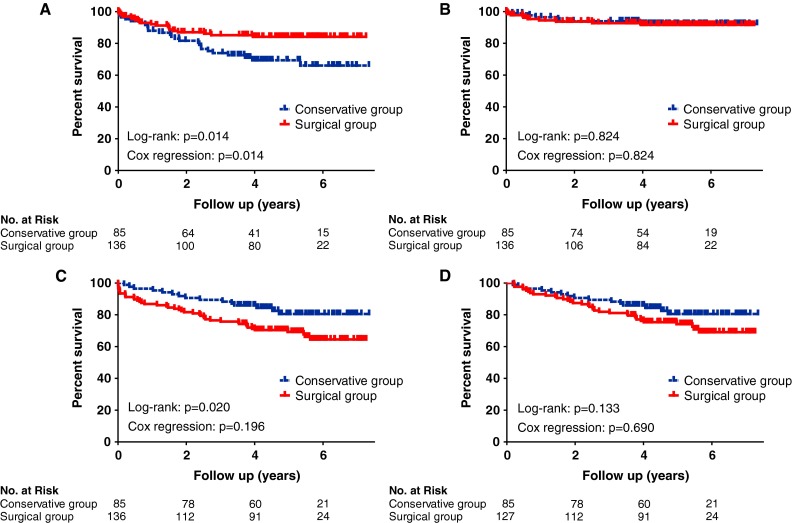
Results: Among 221 patients admitted with SBO, 136 underwent a surgical procedure (surgical group) and 85 were managed conservatively (conservative group). Baseline characteristics were similar between treatment groups. The median follow-up time (interquartile range) was 4.7 (3.7-5.8) years. Nineteen patients (14.0 %) of the surgical group were hospitalized for recurrent SBO versus 25 (29.4 %) of the conservative group [hazard ratio (HR), 0.5; 95 % CI, 0.3-0.9]. The need for a surgical management of a new SBO episode was similar between the two groups, ten patients (7.4 %) in the surgical group and six patients (7.1 %) in the conservative group (HR, 1.1; 95 % CI, 0.4-3.1). Five-year mortality from the date of hospital discharge was not significantly different between the two groups (age- and sex-adjusted HR, 1.1; 95 % CI, 0.6-2.1). A follow-up evaluation was obtained for 130 patients. Among them, 24 patients (34.8 %) of the surgical group and 35 patients (57.4 %) of the conservative group had recurrent SBO symptoms (odds ratio, 0.4; 95 % CI, 0.2-0.8).
Conclusions: The recurrence of SBO symptoms and new hospitalizations were significantly lower after surgical management of SBO compared with conservative treatment.
Figures
References
-
- Nobie B (2012) Small bowel obstruction in emergency medicine. Medscape reference. http://emedicine.medscape.com/article/774140-overview. Accessed 1 Dec 2012
-
- Holzheimer R. Surgical treatment: evidence-based and problem-oriented. Munich: Zuckschwerdt; 2001. - PubMed
-
- Herlinger H. Obstruction. In: Gore RM, Levine MS, Laufer I, editors. Textbook of gastrointestinal radiology. Philadelphia: Saunders; 1994. pp. 931–966.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
