

Efficacy and safety of tenofovir in a kidney transplant patient with chronic hepatitis B and nucleos(t)ide multidrug resistance: a case report
- PMID: 25146249
- PMCID: PMC4155764
- DOI: 10.1186/1752-1947-8-281
Efficacy and safety of tenofovir in a kidney transplant patient with chronic hepatitis B and nucleos(t)ide multidrug resistance: a case report
Abstract
Introduction: Five nucleos(t)ide analogs are used to treat chronic hepatitis B. Ideal nucleos(t)ide analog therapy in chronic hepatitis B patients with kidney transplantation must ensure virological suppression and minimize renal injury. However, resistance to nucleos(t)ide analogs frequently results in virological breakthrough, hepatitis flare, and complicated deterioration of the transplanted kidney. Inappropriate rescue therapy for drug resistance may subsequently cause hepatitis B virus multidrug resistance. Currently, tenofovir is used to treat chronic hepatitis B patients with kidney transplantation. In the field, we first reported combination therapy with tenofovir plus entecavir in a kidney transplant chronic hepatitis B patient with nucleos(t)ide analog multidrug resistance.
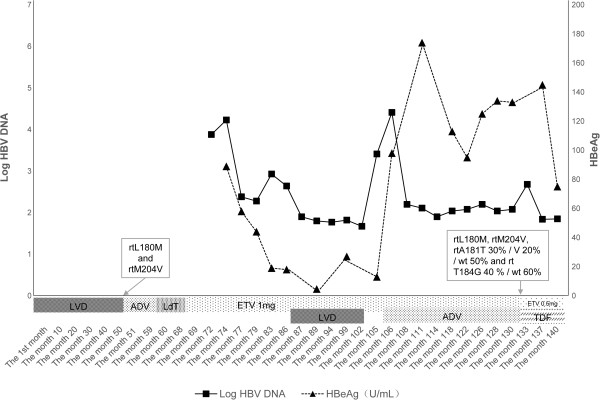
Case presentation: A 50-year-old Chinese man with chronic hepatitis B and kidney transplantation received nucleos(t)ide analog therapy with sequential monotherapy and combination therapy. Virological parameters, hepatic enzymology and renal function were monitored. Drug-resistance mutations were detected by sequence analysis. Our patient received sequential nucleos(t)ide analog monotherapy and inappropriate combination therapy during 132 months, which caused multidrug resistance and renal functional injury. Entecavir plus adefovir was administered in month 106, resulting in decreased hepatitis B virus load, normal hepatic function, and stabilized creatinine clearance. As a result of rebounded viral load and significantly declining creatinine clearance, tenofovir plus entecavir was administered in month 133. After eight weeks, undetectable hepatitis B virus DNA, normal hepatic function and improved creatinine clearance were present. Compared with combination therapy with adefovir plus entecavir, tenofovir plus entecavir showed a potent antiviral effect for multidrug resistance and minimized renal injury.
Conclusions: In chronic hepatitis B patients with kidney transplantation, sequential monotherapy with antiviral agents with low barriers to resistance should be avoided, and initial therapy with entecavir is a better option. Combination therapy with tenofovir plus entecavir in this setting with multidrug resistance is safe and effective.
Figures

Similar articles
-
Mixed treatment comparison meta-analysis evaluating the relative efficacy of nucleos(t)ides for treatment of nucleos(t)ide-naive patients with chronic hepatitis B.Value Health. 2010 Dec;13(8):934-45. doi: 10.1111/j.1524-4733.2010.00777.x. Epub 2010 Sep 3. Value Health. 2010. PMID: 20825624
-
Antiviral effect of entecavir in chronic hepatitis B: influence of prior exposure to nucleos(t)ide analogues.J Hepatol. 2010 Apr;52(4):493-500. doi: 10.1016/j.jhep.2010.01.012. Epub 2010 Feb 4. J Hepatol. 2010. PMID: 20185191 Clinical Trial.
-
Comparison of the efficacy of entecavir and tenofovir in chronic hepatitis B.Hepatogastroenterology. 2012 Mar-Apr;59(114):477-80. doi: 10.5754/hge11426. Hepatogastroenterology. 2012. PMID: 21940383
-
Efficacy of entecavir-tenofovir combination therapy for chronic hepatitis B patients with multidrug-resistant strains.Antimicrob Agents Chemother. 2014 Nov;58(11):6710-6. doi: 10.1128/AAC.03845-14. Epub 2014 Aug 25. Antimicrob Agents Chemother. 2014. PMID: 25155601 Free PMC article.
-
Review article: nucleos(t)ide analogues in patients with chronic hepatitis B virus infection and chronic kidney disease.Aliment Pharmacol Ther. 2014 Jan;39(1):35-46. doi: 10.1111/apt.12538. Epub 2013 Oct 29. Aliment Pharmacol Ther. 2014. PMID: 24299322 Review.
Cited by
-
Clinical Outcomes of Tenofovir Versus Zidovudine-based Regimens Among People Living with HIV/AIDS: a Two Years Retrospective Cohort Study.Open AIDS J. 2017 Jan 23;11:1-11. doi: 10.2174/1874613601711010001. eCollection 2017. Open AIDS J. 2017. PMID: 28217219 Free PMC article.
-
Adverse effects of oral antiviral therapy in chronic hepatitis B.World J Hepatol. 2017 Feb 18;9(5):227-241. doi: 10.4254/wjh.v9.i5.227. World J Hepatol. 2017. PMID: 28261380 Free PMC article. Review.
-
New therapeutic options for persistent low-level viremia in patients with chronic hepatitis B virus infection: Increase of entecavir dosage.World J Gastroenterol. 2021 Feb 28;27(8):666-676. doi: 10.3748/wjg.v27.i8.666. World J Gastroenterol. 2021. PMID: 33716446 Free PMC article. Review.
-
Tenofovir and kidney transplantation: case report.Clin Nephrol Case Stud. 2016 Aug 29;4:18-23. doi: 10.5414/CNCS108929. eCollection 2016. Clin Nephrol Case Stud. 2016. PMID: 29043137 Free PMC article.
References
-
- Papatheodoridis G, Buti M, Cornberg M, Janssen HL, Mutimer D, Pol S, Raimondo G, Dusheiko G, Lok A, Marcellin P. EASL clinical practice guidelines: Management of chronic hepatitis B virus infection. J Hepatol. 2012;57:167–185. - PubMed
-
- Liaw YF, Leung N, Kao JH, Piratvisuth T, Gane E, Han KH, Guan R, Lau GK, Locarnini S. Chronic Hepatitis B Guideline Working Party of the Asian-Pacific Association for the Study of the Liver. Asian-Pacific consensus statement on the management of chronic hepatitis B: a 2008 update. Hepatol Int. 2008;2:263–283. doi: 10.1007/s12072-008-9080-3. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
