

Response of day-to-day home blood pressure variability by antihypertensive drug class after transient ischemic attack or nondisabling stroke
- PMID: 25147330
- PMCID: PMC5447806
- DOI: 10.1161/STROKEAHA.114.005982
Response of day-to-day home blood pressure variability by antihypertensive drug class after transient ischemic attack or nondisabling stroke
Abstract
Background and purpose: Visit-to-visit variability in systolic blood pressure (SBP) is associated with an increased risk of stroke and was reduced in randomized trials by calcium channel blockers and diuretics but not by renin-angiotensin system inhibitors. However, time of day effects could not be determined. Day-to-day variability on home BP readings predicts stroke risk and potentially offers a practical method of monitoring response to variability-directed treatment.
Methods: SBP mean, maximum, and variability (coefficient of variation=SD/mean) were determined in 500 consecutive transient ischemic attack or minor stroke patients on 1-month home BP monitoring (3 BPs, 3× daily). Hypertension was treated to a standard protocol. Differences in SBP variability from 3 to 10 days before to 8 to 15 days after starting or increasing calcium channel blockers/diuretics versus renin-angiotensin system inhibitors versus both were compared by general linear models, adjusted for risk factors and baseline BP.
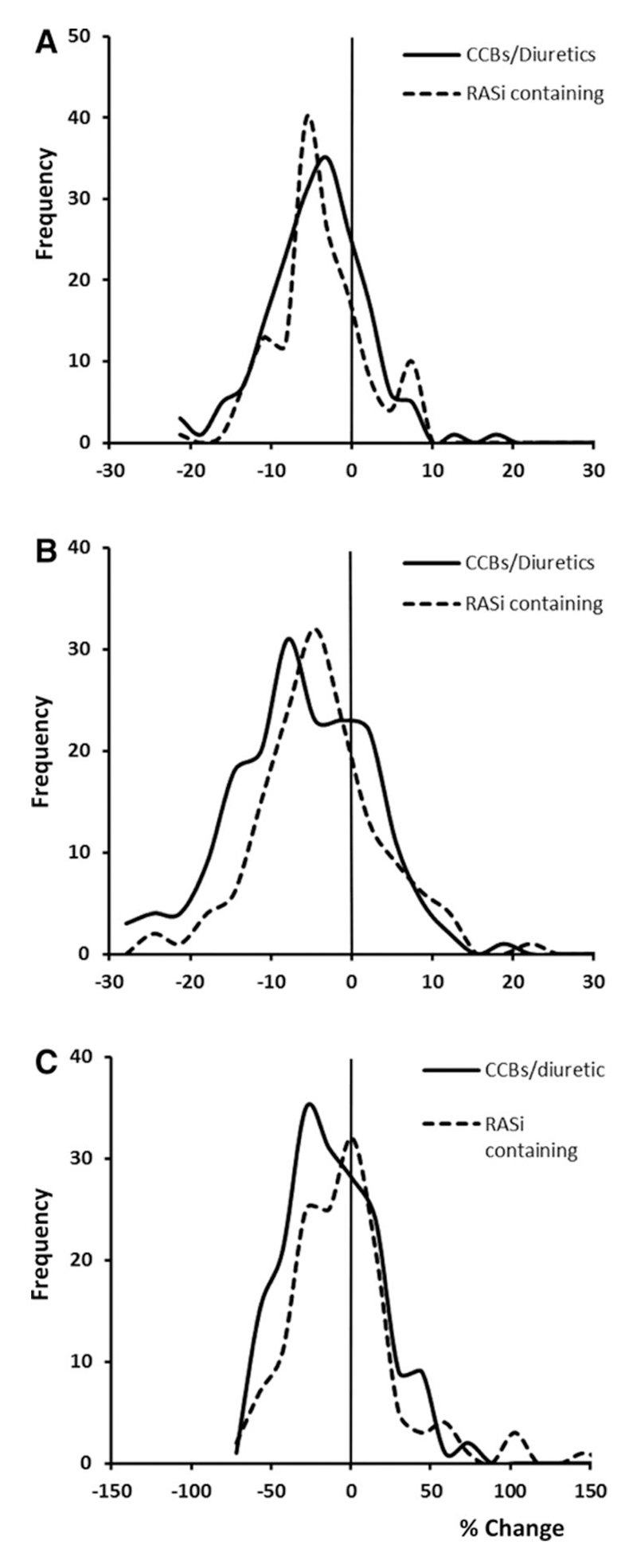
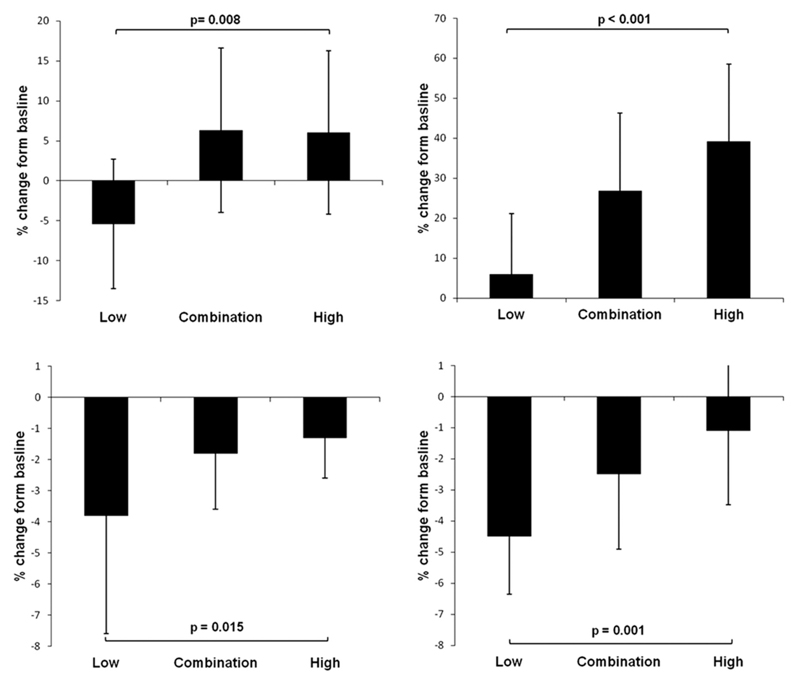
Results: Among 288 eligible interventions, variability in SBP was reduced after increased treatment with calcium channel blockers/diuretics versus both versus renin-angiotensin system inhibitors (-4.0 versus 6.9 versus 7.8%; P=0.015), primarily because of effects on maximum SBP (-4.6 versus -1.0 versus -1.0%; P=0.001), with no differences in effect on mean SBP. Class differences were greatest for early-morning SBP variability (3.6 versus 17.0 versus 38.3; P=0.002) and maximum (-4.8 versus -2.0 versus -0.7; P=0.001), with no effect on midmorning (P=0.29), evening (P=0.65), or diurnal variability (P=0.92).
Conclusions: After transient ischemic attack or minor stroke, calcium channel blockers and diuretics reduced variability and maximum home SBP, primarily because of effects on morning readings. Home BP readings enable monitoring of response to SBP variability-directed treatment in patients with recent cerebrovascular events.
Keywords: antihypertensive agents; home blood pressure monitoring; stroke.
© 2014 American Heart Association, Inc.
Figures
References
-
- Rothwell PM. Limitations of the usual BP hypothesis and importance of variability, instability, and episodic hypertension. Lancet. 2010;375:938–948. - PubMed
-
- Rothwell PM, Howard SC, Dolan E, O’Brien E, Dobson JE, Dahlof B, et al. Prognostic significance of visit-to-visit variability, maximum systolic BP, and episodic hypertension. Lancet. 2010;375:895–905. - PubMed
-
- Rothwell PM, Howard SC, Dolan E, O’Brien E, Dobson JR, Dahlof B, et al. Effects of β blockers and calcium-channel blockers on within-individual variability in BP and risk of stroke. Lancet Neurology. 2010;9:469–480. - PubMed
-
- Webb AJS, Fischer U, Mehta Z, Rothwell PM. Effects of antihypertensive-drug class on interindividual variation in BP and risk of stroke. Lancet. 2010;375:906–915. - PubMed
-
- Webb AJ, Fischer U, Rothwell PM. Effects of beta-blocker selectivity on blood pressure variability and stroke: a systematic review. Neurology. 2011;77:731–737. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
