

Dynamics of lung defense in pneumonia: resistance, resilience, and remodeling
- PMID: 25148693
- PMCID: PMC4366440
- DOI: 10.1146/annurev-physiol-021014-071937
Dynamics of lung defense in pneumonia: resistance, resilience, and remodeling
Abstract
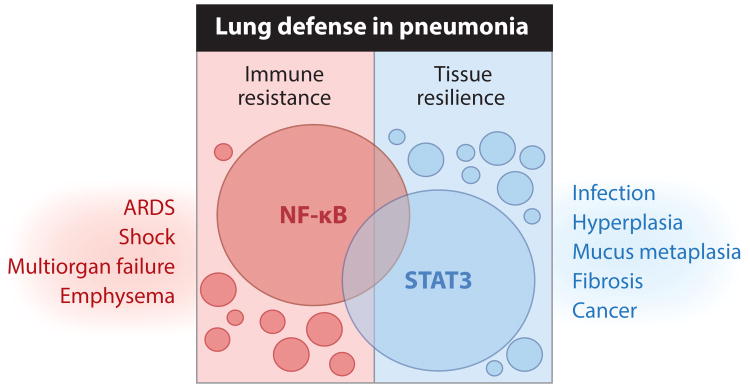
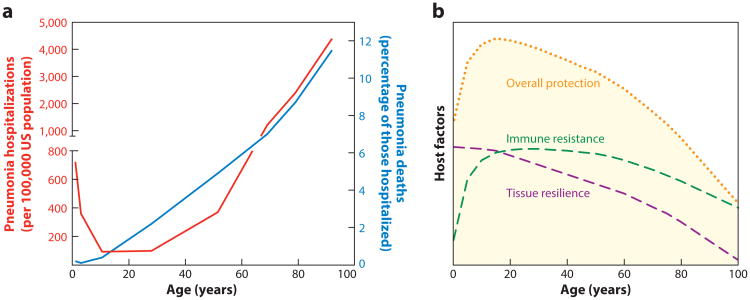
Pneumonia is initiated by microbes in the lung, but physiological processes integrating responses across diverse cell types and organ systems dictate the outcome of respiratory infection. Resistance, or actions of the host to eradicate living microbes, in the lungs involves a combination of innate and adaptive immune responses triggered by air-space infection. Resilience, or the ability of the host tissues to withstand the physiologically damaging effects of microbial and immune activities, is equally complex, precisely regulated, and determinative. Both immune resistance and tissue resilience are dynamic and change throughout the lifetime, but we are only beginning to understand such remodeling and how it contributes to the incidence of severe pneumonias, which diminishes as childhood progresses and then increases again among the elderly. Here, we review the concepts of resistance, resilience, and remodeling as they apply to pneumonia, highlighting recent advances and current significant knowledge gaps.
Keywords: NF-κB; STAT3; cytokines; innate immunity; lung; respiratory infection.
Figures
References
-
- Armstrong GL, Conn LA, Pinner RW. Trends in infectious disease mortality in the United States during the 20th century. JAMA. 1999;281:61–66. - PubMed
-
- Liu L, Johnson HL, Cousens S, Perin J, Scott S, et al. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet. 2012;379:2151–61. - PubMed
-
- Curns AT, Holman RC, Sejvar JJ, Owings MF, Schonberger LB. Infectious disease hospitalizations among older adults in the United States from 1990 through 2002. Arch Intern Med. 2005;165:2514–20. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
