

Successful treatment of recurrent cholangitis by constructing a hepaticojejunostomy with long Roux-en-Y limb in a long-term surviving patient after a Whipple procedure for pancreatic adenocarcinoma
- PMID: 25150551
- PMCID: PMC4152249
- DOI: 10.12659/AJCR.890436
Successful treatment of recurrent cholangitis by constructing a hepaticojejunostomy with long Roux-en-Y limb in a long-term surviving patient after a Whipple procedure for pancreatic adenocarcinoma
Abstract
Patient: Female, 74.
Final diagnosis: Recurrent cholangitis.
Symptoms: -.
Medication: -.
Clinical procedure: -.
Specialty: Gastroenterology and Hepatology.
Objective: Unusual clinical course.
Background: Cholangitis may result from biliary obstruction (e.g., biliary or anastomotic stenosis, or foreign bodies) or occur in the presence of normal biliary drainage. Although reflux of intestinal contents into the biliary tree after hepaticojejunostomy appears to be a rare complication, it is important to emphasize that there are few available surgical therapeutic techniques.
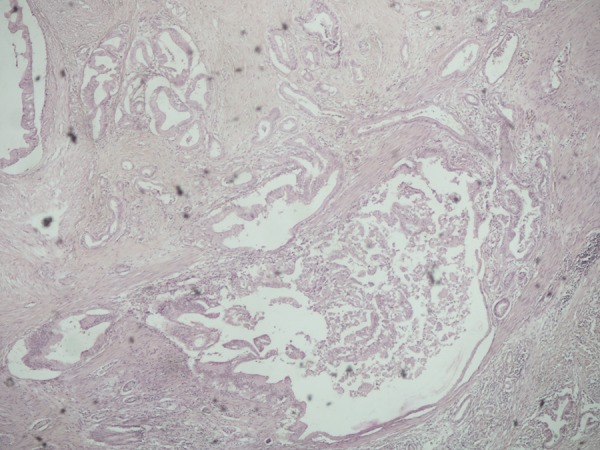
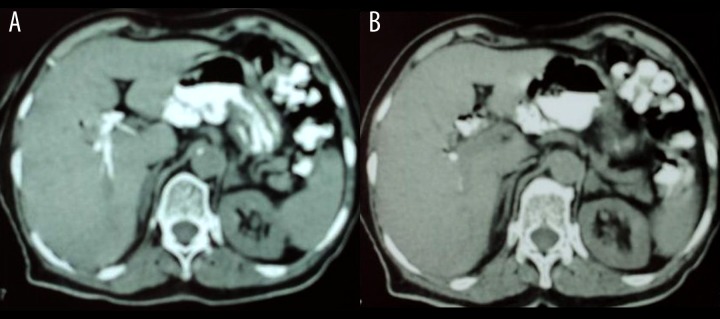
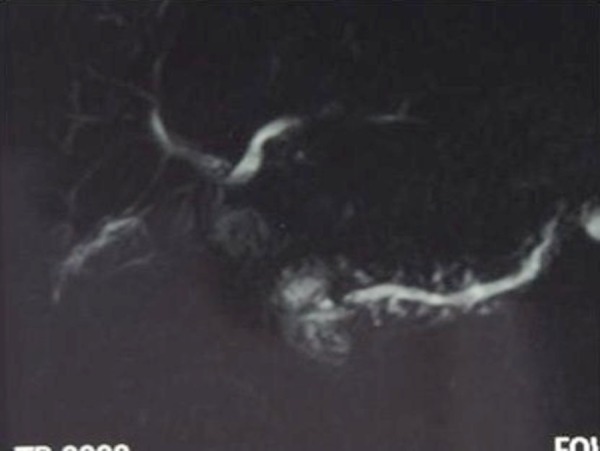
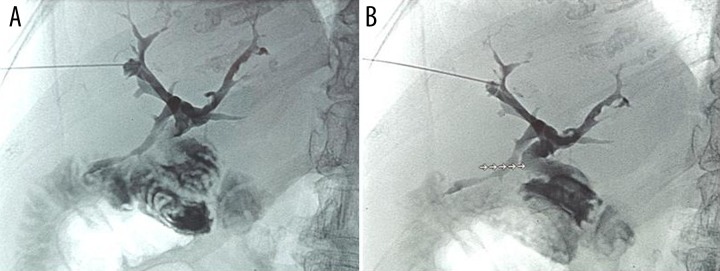
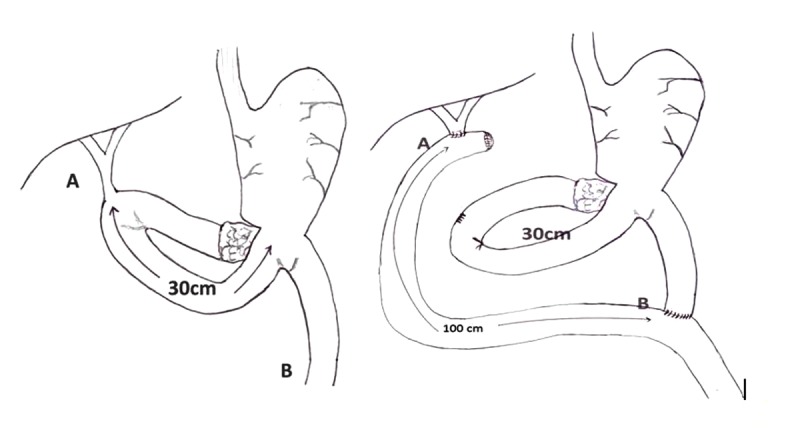
Case report: A 74-year-old woman presented to our hospital after 17 years of episodes of cholangitis. The patient had undergone a pancreatoduodenectomy (Whipple procedure) 18 years earlier due to pancreatic adenocarcinoma. The reconstruction was achieved through the sequential placement of pancreatic, biliary, and retrocolic gastric anastomosis into the same jejunal loop. The postoperative course was uneventful and the patient received adjuvant chemotherapy. Approximately 6 months after the initial operation, the patient started having episodes of cholangitis. Over the next 17 years she experienced several febrile episodes presumed to be secondary to cholangitis. A computing tomography (CT) scan of the abdomen revealed intrahepatic bile ducts partially filled with orally administered contrast material (Gastrografin). Magnetic resonance cholangiopancreatography (MRCP) showed dilatation of the left intrahepatic bile ducts. A percutaneous transhepatic cholangiography showed that the bilioenteric anastomosis was normal, without stenosis. Based on these findings, a diagnosis of a short loop between the hepaticojejunostomy and the gastrojejunostomy permitting the reflux of intestinal juice into the biliary tree was made. During the re-operation, a new hepaticojejunal anastomosis in a 100-cm long Roux-en-Y loop was performed to prevent the reflux of the intestinal fluid into the biliary tree. The patient was discharged on postoperative day 10. One year after the second procedure, the patient enjoys good health and has been free of fever and abdominal pain and has not received any antibiotic therapy.
Conclusions: Lengthening the efferent Roux-en-Y limb should be considered as a therapeutic option when treating a patient with recurrent episodes of cholangitis after hepaticojejunostomy.
Figures
References
-
- Chuang JH, Lee SY, Chen WJ, et al. Changes in bacterial concentration in the liver correlate with that in the hepaticojejunostomy after bile duct reconstruction: implication in the pathogenesis of postoperative cholangitis. World J Surg. 2001;25:1512–18. - PubMed
-
- Lasnier C, Kohneh-Shahri N, Paineau J. Dysfonctionnement des anastomoses biliodigestives: à propos d’unesériechirurgicale de 20 cas. Revue de la littérature. Ann de Chirourgie. 2005;130:566–72. [in French] - PubMed
-
- Stewart L, Way LW. Bile duct injuries during laparoscopic cholecystectomy.Factors that influence the results of treatment. Arch Surg. 1995;130:1123–29. - PubMed
-
- Casendes A, Navarrete C, Burdiles P, Yarmuch J. Treatment of common bile duct injuries during laparoscopic cholecystectomy: endoscopic and surgical management. World J Surg. 2001;25:1346–51. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
