

The role of the microbiome in exacerbations of chronic lung diseases
- PMID: 25152271
- PMCID: PMC4166502
- DOI: 10.1016/S0140-6736(14)61136-3
The role of the microbiome in exacerbations of chronic lung diseases
Abstract
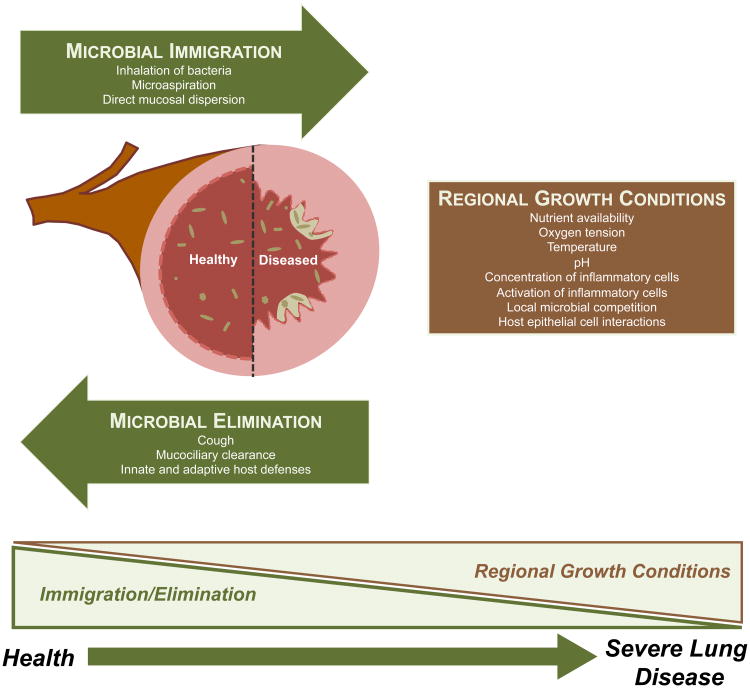
Culture-independent microbiological techniques have shown a previously unappreciated complexity to the bacterial microbiome of the respiratory tract that forces reconsideration of the interactions between host, bacteria, and the pathogenesis of exacerbations of chronic lung disease. The composition of the lung microbiome is determined by microbial immigration, elimination, and relative growth rates of its members. All these factors change dramatically in chronic lung disease and further during exacerbations. Exacerbations lack the features of bacterial infections, including increased bacterial burden and decreased diversity of microbial communities. We propose that exacerbations are occasions of respiratory tract dysbiosis--a disorder of the respiratory tract microbial ecosystem with negative effects on host biology. Respiratory tract dysbiosis provokes a dysregulated host immune response, which in turn alters growth conditions for microbes in airways, promoting further dysbiosis and perpetuating a cycle of inflammation and disordered microbiota. Differences in the composition of baseline respiratory tract microbiota might help to explain the so-called frequent-exacerbator phenotype observed in several disease states, and might provide novel targets for therapeutic intervention.
Copyright © 2014 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Figures



References
-
- Strassels SA, Smith DH, Sullivan SD, Mahajan PS. The costs of treating COPD in the United States. Chest. 2001;119(2):344–52. - PubMed
-
- Smith DH, Malone DC, Lawson KA, Okamoto LJ, Battista C, Saunders WB. A national estimate of the economic costs of asthma. Am J Respir Crit Care Med. 1997;156(3 Pt 1):787–93. - PubMed
-
- Lieu TA, Ray GT, Farmer G, Shay GF. The cost of medical care for patients with cystic fibrosis in a health maintenance organization. Pediatrics. 1999;103(6):e72. - PubMed
-
- Seemungal TA, Donaldson GC, Bhowmik A, Jeffries DJ, Wedzicha JA. Time course and recovery of exacerbations in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2000;161(5):1608–13. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
