

Main causes and diagnostic evaluation in patients with primary complaint of olfactory disturbances
- PMID: 25153103
- PMCID: PMC9535487
- DOI: 10.1016/j.bjorl.2014.02.001
Main causes and diagnostic evaluation in patients with primary complaint of olfactory disturbances
Abstract
Introduction: Establishing a diagnosis in patients with olfactory disturbances has always been challenging for physicians.One reason for this is the rarity of some of the diseases that affect this sense, such as Kallmann's syndrome and post-viral olfactory loss.
Objective: To identify the major causes of olfactory disturbances and to describe the diagnostic evaluation in outpatients attended to at an ambulatory clinic specialized in olfaction disorders.
Methods: A retrospective analysis was performed in outpatients with primary olfactory complaint attended to between June 1, 2011 and September 30, 2013 in a center specialized in olfactory disorders. Patient history, nasofibroscopy, and the University of Pennsylvania Smell Identification Test (UPSIT) comprised the examination.
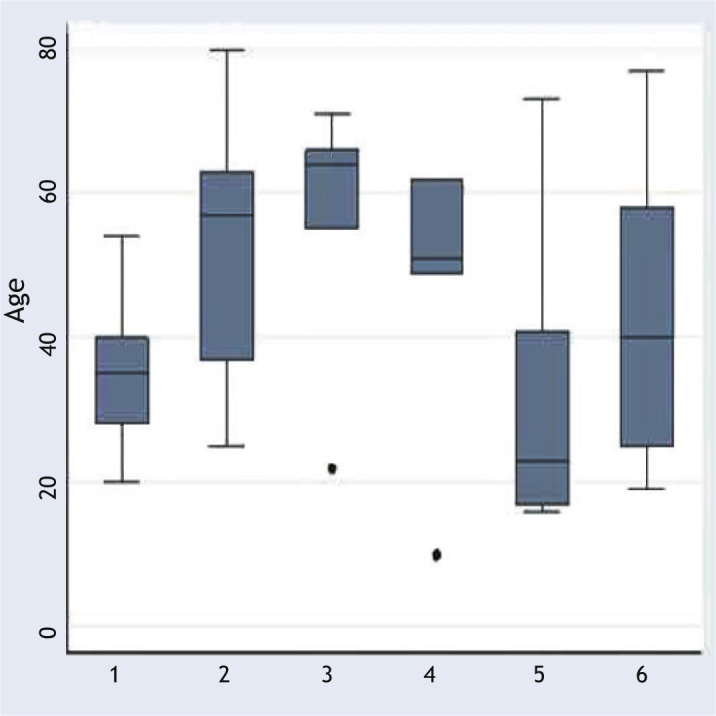
Results: Sixty-two patients were evaluated. The major causes were chronic rhinosinusitis (31%); rhinitis, primarily the allergic type (19%); post-viral olfactory loss (13%); and post-traumatic loss (8%). UPSIT scores were statistically different among different etiologies (p = 0.01).
Conclusions: The major diagnoses that should be part of the physician assessment when a patient complains of olfactory disturbance are chronic rhinosinusitis with and without polyps, allergic rhinitis, post-viral olfactory loss, and post-traumatic loss.
Introdução: Estabelecer um diagnóstico em pacientes com distúrbios olfatórios foi sempre um desafio aos médicos. Uma das razões para isso é a raridade de algumas doenças que afetam esse sentido como a Síndrome de Kallmann e a perda olfatória pós-viral.
Objetivo: Identificar as principais causas das doenças olfatórias e descrever sua condução diagnóstica em um ambulatório direcionado a esses distúrbios.
Método: Análise retrospectiva de pacientes ambulatoriais com queixa olfatória primária atendida entre 1° de junho de 2011 e 30 de setembro de 2013 em centro especializado. História clínica, nasofibroscopia e o Teste de Identificação do Olfato da Universidade da Pensilvânia (UPSIT) compuseram a avaliação. Sempre que necessário, foram solicitadas tomografia de seios paranasais e ressonância magnética de crânio.
Resultados: Sessenta e dois pacientes foram avaliados. As causas mais comuns encontradas foram respectivamente: rinossinusite crônica (31%), rinites (19%), principalmente a rinite alérgica, perda olfatória pós-viral (13%) e pós-traumática (8%). As pontuações no UPSIT foram estatisticamente diferentes entre as cinco principais causas (p = 0,01).
Conclusões: Os principais diagnósticos que devem fazer parte na investigação médica diante de um paciente com queixa olfatória são: rinossinusite crônica com e sem polipose nasal, rinite alérgica, perda olfatória pós-viral e pós-traumática.
Figures
Similar articles
-
The diagnosis of a conductive olfactory loss.Laryngoscope. 2001 Jan;111(1):9-14. doi: 10.1097/00005537-200101000-00002. Laryngoscope. 2001. PMID: 11192906
-
Fluctuating olfactory sensitivity and distorted odor perception in allergic rhinitis.Arch Otolaryngol Head Neck Surg. 1999 Sep;125(9):1005-10. doi: 10.1001/archotol.125.9.1005. Arch Otolaryngol Head Neck Surg. 1999. PMID: 10488987
-
Some abnormalities of smell.J Laryngol Otol. 1970 Dec;84(12):1185-91. doi: 10.1017/s0022215100072935. J Laryngol Otol. 1970. PMID: 5491643 No abstract available.
-
An updated review of clinical olfaction.Curr Opin Otolaryngol Head Neck Surg. 2006 Feb;14(1):23-8. doi: 10.1097/01.moo.0000193174.77321.39. Curr Opin Otolaryngol Head Neck Surg. 2006. PMID: 16467634 Review.
-
Temporary olfactory improvement in chronic rhinosinusitis with nasal polyps after treatment.Eur Arch Otorhinolaryngol. 2018 Sep;275(9):2193-2202. doi: 10.1007/s00405-018-5066-5. Epub 2018 Jul 19. Eur Arch Otorhinolaryngol. 2018. PMID: 30027441 Review.
Cited by
-
Chemosensory Dysfunction in COVID-19: Prevalences, Recovery Rates, and Clinical Associations on a Large Brazilian Sample.Otolaryngol Head Neck Surg. 2021 Mar;164(3):512-518. doi: 10.1177/0194599820954825. Epub 2020 Sep 1. Otolaryngol Head Neck Surg. 2021. PMID: 32867582 Free PMC article.
-
Is SARS-CoV-2 (COVID-19) postviral olfactory dysfunction (PVOD) different from other PVOD?World J Otorhinolaryngol Head Neck Surg. 2020 Nov;6(Suppl 1):S26-S32. doi: 10.1016/j.wjorl.2020.05.004. Epub 2020 May 19. World J Otorhinolaryngol Head Neck Surg. 2020. PMID: 32837756 Free PMC article. Review.
-
V Brazilian Consensus on Rhinitis - 2024.Braz J Otorhinolaryngol. 2025 Jan-Feb;91(1):101500. doi: 10.1016/j.bjorl.2024.101500. Epub 2024 Sep 7. Braz J Otorhinolaryngol. 2025. PMID: 39388827 Free PMC article. Review.
-
A new biomarker combining multimodal MRI radiomics and clinical indicators for differentiating inverted papilloma from nasal polyp invaded the olfactory nerve possibly.Front Neurol. 2023 Mar 21;14:1151455. doi: 10.3389/fneur.2023.1151455. eCollection 2023. Front Neurol. 2023. PMID: 37025198 Free PMC article.
-
Olfactory nerve: from ugly duckling to swan.Arq Neuropsiquiatr. 2022 Jan;80(1):75-83. doi: 10.1590/0004-282X-ANP-2020-0529. Arq Neuropsiquiatr. 2022. PMID: 35239810 Free PMC article. Review.
References
-
- Deems D.A., Doty R.L., Settle R.G., Moore-Gillon V., Shaman P., Mester A.F., et al. Smell and taste disorders, a study of 750 patients from the University of Pennsylvania Smell and Taste Center. Arch Otolaryngol Head Neck Surg. 1991;117:519–528. - PubMed
-
- Harris R., Davidson T.M., Murphy C., Gilbert P.E., Chen M. Clinical evaluation and symptoms of chemosensory impairment: one thousand consecutive cases from the Nasal Dysfunction Clinic in San Diego. Am J Rhinol. 2006;20:101–108. - PubMed
-
- Nordin S., Murphy C., Davidson T.M., Quiñonez C., Jalowayski A.A., Ellison D.W. Prevalence and assessment of qualitative olfactory dysfunction in different age groups. Laryngoscope. 1996;106:739–744. - PubMed
-
- Seiden A.M., Duncan H.J. The diagnosis of a conductive olfactory loss. Laryngoscope. 2001;111:9–14. - PubMed
-
- Lin S.H., Chu S.T., Yuan B.C., Suh C.H. Survey of the frequency of olfactory dysfunction in Taiwan. J Chin Med Assoc. 2009;72:68–71. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
