

Human cytomegalovirus infection in tumor cells of the nervous system is not detectable with standardized pathologico-virological diagnostics
- PMID: 25155358
- PMCID: PMC4201076
- DOI: 10.1093/neuonc/nou167
Human cytomegalovirus infection in tumor cells of the nervous system is not detectable with standardized pathologico-virological diagnostics
Abstract
Background: Experimental findings have suggested that human cytomegalovirus (HCMV) infection of tumor cells may exert oncomodulatory effects that enhance tumor malignancy. However, controversial findings have been published on the presence of HCMV in malignant tumors. Here, we present the first study that systematically investigates HCMV infection in human nervous system tumors by highly sensitive immunohistochemistry in correlation with the HCMV serostatus of the patients.
Methods: Immunohistochemical and quantitative PCR-based methods to detect different HCMV antigens and genomic HCMV DNA were optimized prior to the investigation of pathological samples. Moreover, the pathological results were matched with the HCMV serostatus of the patients.
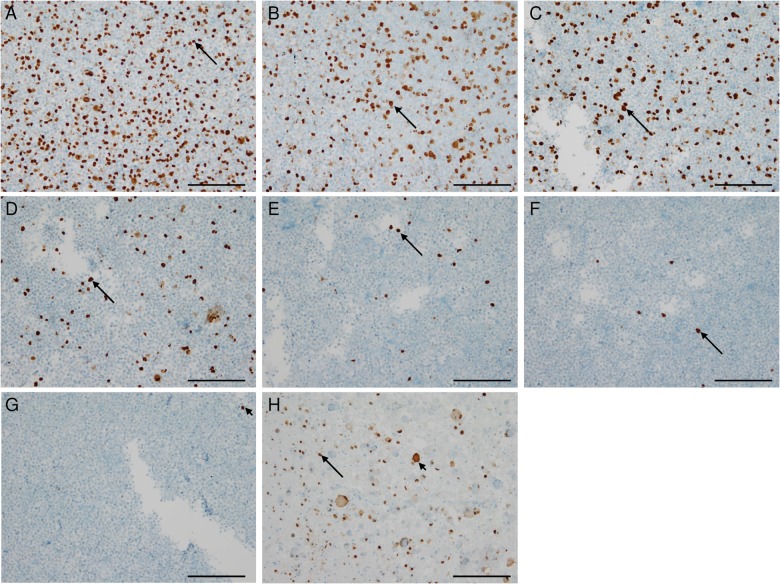
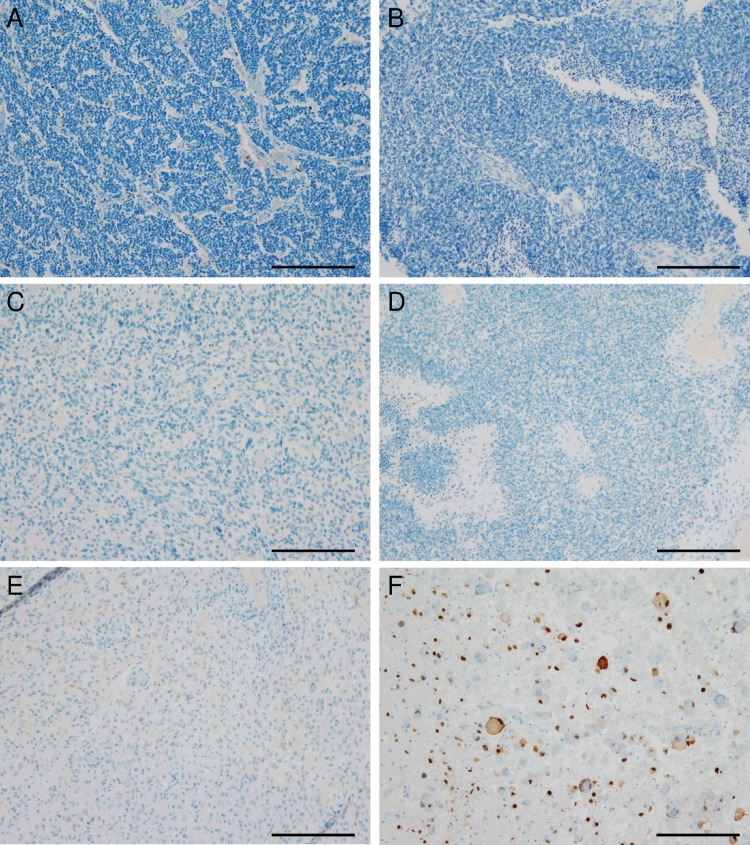
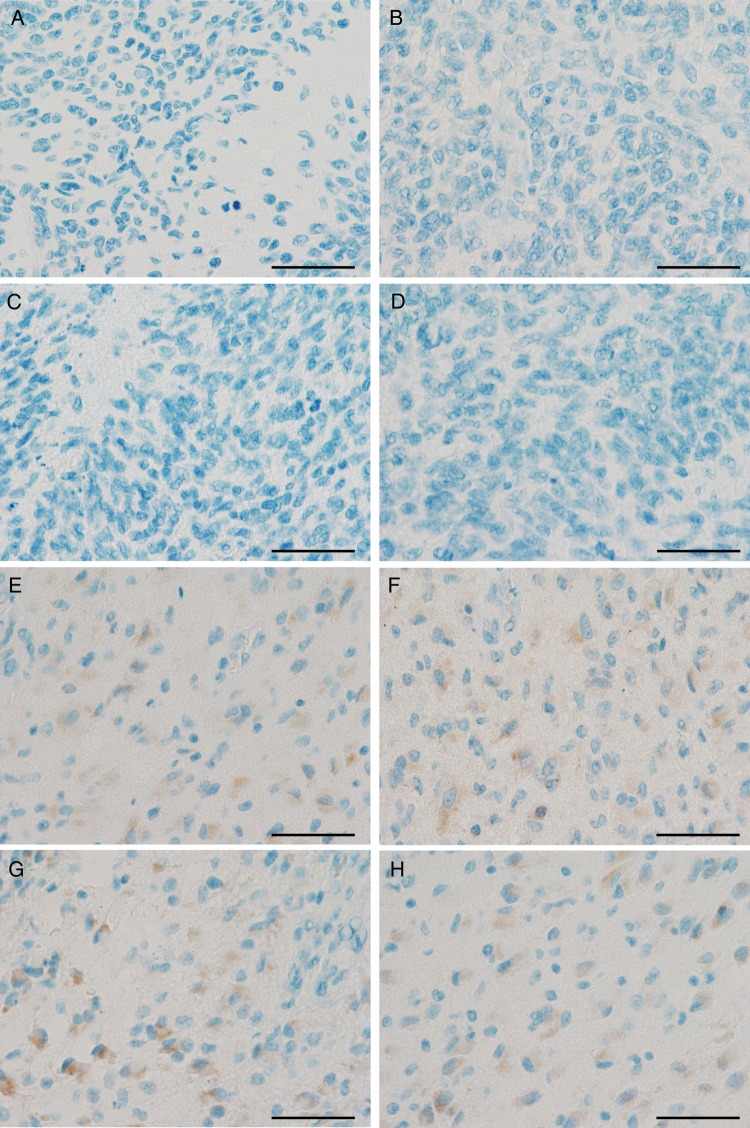
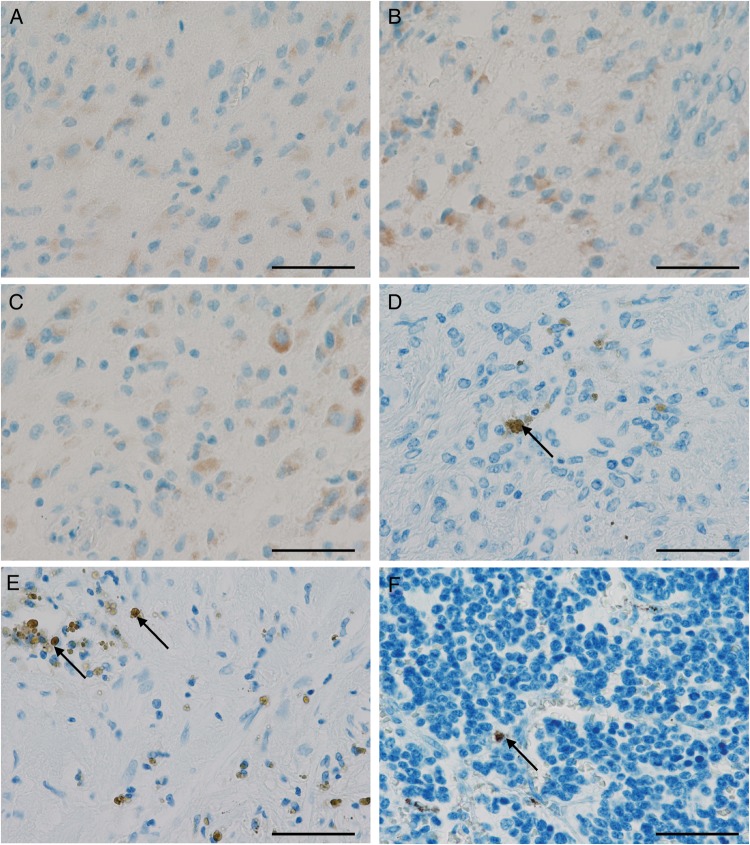
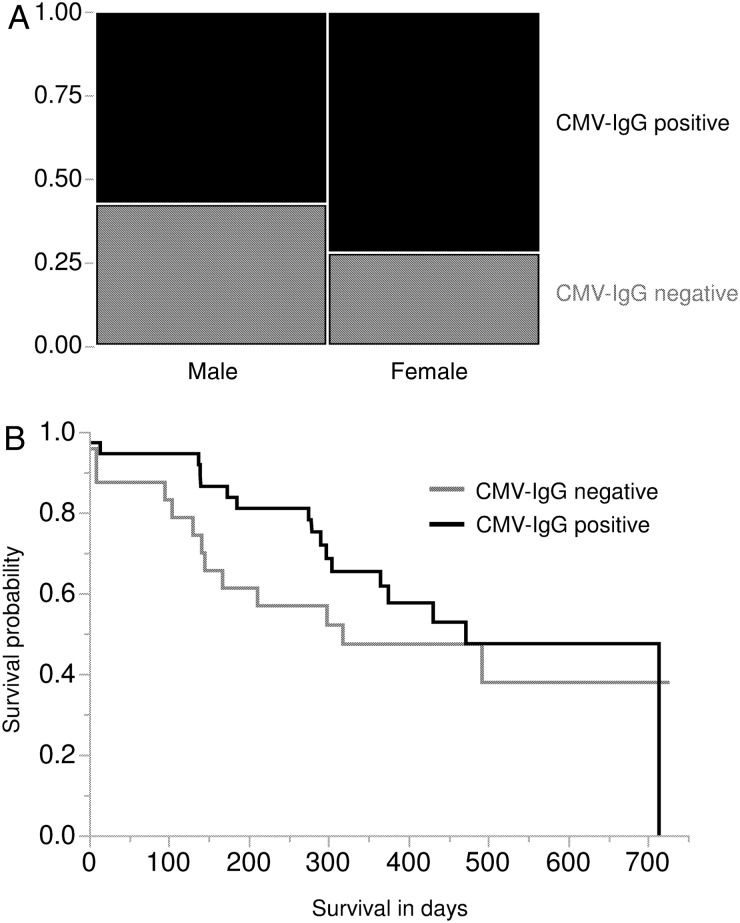
Results: HCMV immediate-early, late, and pp65 antigens could be detected in single cells from HCMV strain Hi91-infected UKF-NB-4 neuroblastoma cells after 1:1024 dilution with noninfected UKF-NB-4 cells. Genomic HCMV DNA could be detected in copy numbers as low as 430 copies/mL. However, we did not detect HCMV in tumors from a cohort of 123 glioblastoma, medulloblastoma, or neuroblastoma patients. Notably, we detected nonspecifically positive staining in tumor tissues of HCMV seropositive and seronegative glioblastoma patients. The HCMV serostatus of 67 glioblastoma patients matched the general epidemiological prevalence data for Western countries (72% of female and 57% of male glioblastoma patients were HCMV seropositive). Median survival was not significantly different in HCMV seropositive versus seronegative glioblastoma patients.
Conclusions: The prevalence of HCMV-infected tumor cells may be much lower than previously reported based on highly sensitive detection methods.
Keywords: cytomegalovirus; glioma; oncomodulation.
© The Author(s) 2014. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Response to "Human cytomegalovirus infection in tumor cells of the nervous system is not detectable with standardized pathologico-virological diagnostics".Neuro Oncol. 2014 Nov;16(11):1435-6. doi: 10.1093/neuonc/nou295. Epub 2014 Oct 13. Neuro Oncol. 2014. PMID: 25313192 Free PMC article. No abstract available.
-
CMV and glioma--are we there yet?Neuro Oncol. 2014 Nov;16(11):1433-4. doi: 10.1093/neuonc/nou296. Neuro Oncol. 2014. PMID: 25326550 Free PMC article. No abstract available.
References
-
- Cannon MJ, Schmid DS, Hyde TB. Review of cytomegalovirus seroprevalence and demographic characteristics associated with infection. Rev Med Virol. 2010;20(4):202–213. - PubMed
-
- Sinclair J. Human cytomegalovirus: latency and reactivation in the myeloid lineage. J Clin Virol. 2008;41:180–185. - PubMed
-
- Mocarski ES, Shenk T, Pass RF. Cytomegaloviruses. In: Knipe DM, Howley PM, editors. Fields Virology. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007. pp. 2701–2772.
-
- Cinatl J, Jr, Cinatl J, Vogel JU, et al. Modulatory effects of human cytomegalovirus infection on malignant properties of cancer cells. Intervirology. 1996;39(4):259–269. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
