

doi: 10.1093/eurheartj/ehu320.
Epub 2014 Aug 24.
Terminology and definition of changes renal function in heart failure
Affiliations
- PMID: 25157110
- PMCID: PMC4375406
- DOI: 10.1093/eurheartj/ehu320
Item in Clipboard
Terminology and definition of changes renal function in heart failure
Eur Heart J.
.
No abstract available
Figures
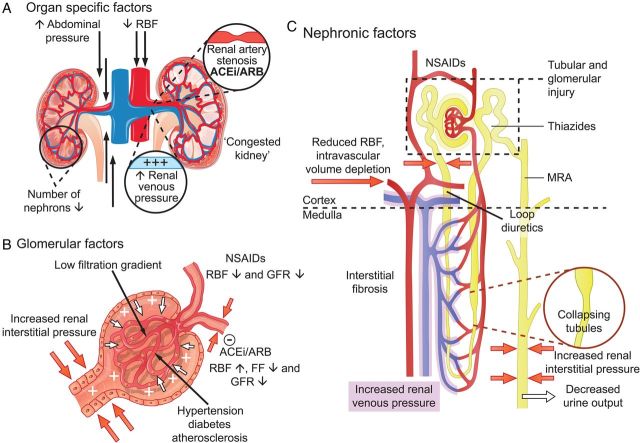
Factors involved in the cause and association with an outcome of changes in renal function in heart failure. (A) Organ-specific factors. The main determinants of decreased glomerular filtration rate are a decrease in renal blood flow and an increase in central and renal venous pressure. The latter can be caused by intravascular congestion, but also by an increase in intra-abdominal pressure. Owing to increased renal venous pressure, renal interstitial pressure rises, which results a ‘congested kidney’ since the kidney is encapsulated (B and C). Renal artery stenosis is present in ∼25% of heart failure patients, which can further compromise renal blood flow, especially in the presence of renin–angiotensin–aldosterone system inhibitors. (B) Glomerular factors. Decreased renal blood flow and low blood pressure trigger renal autoregulation, preserving glomerular filtration rate by increasing filtration fraction by increased efferent vasoconstriction. The use of renin–angiotensin–aldosterone system-inhibitors inhibits this process, which increases renal blood flow, but leads (in some patients) to a reduction in glomerular filtration rate (pseudo-worsening renal function). Non-steroidal anti-inflammatory drugs inhibit prostaglandin synthesis, thereby impairing prostaglandin associated increase/dependent renal blood flow. Increased interstitial pressure causes increased pressure in Bowman's capsule, which directly opposes filtration, in a glomerulus where the filtration gradient is already low due to a decreased renal blood flow and increased renal venous pressure. Concomitant diseases have direct, but differential effect on glomerular filtration, glomerular integrity and podocyte function, as well as autoregulation. (C) Nephronic factors. Different therapies have different renal effects and exert their action at specific sites as indicated in this diagram. Intravascular volume depletion (in the presence or absence of congestion) can lead to impaired renal perfusion and decreased glomerular filtration rate. The combination of increased interstitial pressure, reduced arterial perfusion, concomitant disease and therapies can cause tubular and glomerular injury. Increased renal venous pressure causes increased renal interstitial pressure, resulting in collapsing of renal tubules, which decreases glomerular filtration rate, and eventually leads to decreased urine output, sodium retention, and congestion. ACEi, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; FF, filtration fraction; GFR, glomerular filtration rate; MRA, mineralocorticoid receptor antagonist; NSAIDs, non-steroidal anti-inflammatory drugs; RAAS, renin–angiotensin–aldosterone system; RBF, renal blood flow.
References
-
- Damman K, Valente MA, Voors AA, O'Connor CM, van Veldhuisen DJ, Hillege HL. Renal impairment, worsening renal function, and outcome in patients with heart failure: an updated meta-analysis. Eur Heart J. 2014;35:455–446. - PubMed
-
- Ronco C, McCullough P, Anker SD, Anand I, Aspromonte N, Bagshaw SM, Bellomo R, Berl T, Bobek I, Cruz DN, Daliento L, Davenport A, Haapio M, Hillege H, House AA, Katz N, Maisel A, Mankad S, Zanco P, Mebazaa A, Palazzuoli A, Ronco F, Shaw A, Sheinfeld G, Soni S, Vescovo G, Zamperetti N, Ponikowski P. Acute Dialysis Quality Initiative (ADQI) consensus group. Cardio-renal syndromes: report from the consensus conference of the acute dialysis quality initiative. Eur Heart J. 2010;31:703–711. - PMC - PubMed
-
- Damman K, Voors AA, Navis G, van Veldhuisen DJ, Hillege HL. The cardiorenal syndrome in heart failure. Prog Cardiovasc Dis. 2011;54:14–53. - PubMed
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl. 2012;2:1–138.
-
- Van der Meer P, Postmus D, Ponikowski P, Cleland JG, O'Connor CM, Cotter G, Metra M, Davison BA, Givertz MM, Mansoor GA, Teerlink JR, Massie BM, Hillege HL, Voors AA. The predictive value of short-term changes in hemoglobin concentration in patients presenting with acute decompensated heart failure. J Am Coll Cardiol. 2013;61:1973–1981. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
