

Rare variants in PPARG with decreased activity in adipocyte differentiation are associated with increased risk of type 2 diabetes
- PMID: 25157153
- PMCID: PMC4246964
- DOI: 10.1073/pnas.1410428111
Rare variants in PPARG with decreased activity in adipocyte differentiation are associated with increased risk of type 2 diabetes
Erratum in
- Proc Natl Acad Sci U S A. 2014 Nov;11;111(45):16225. Estrada, Karol [added]; Mercader, Josep [added]; MacArthur, Daniel [added]
Abstract
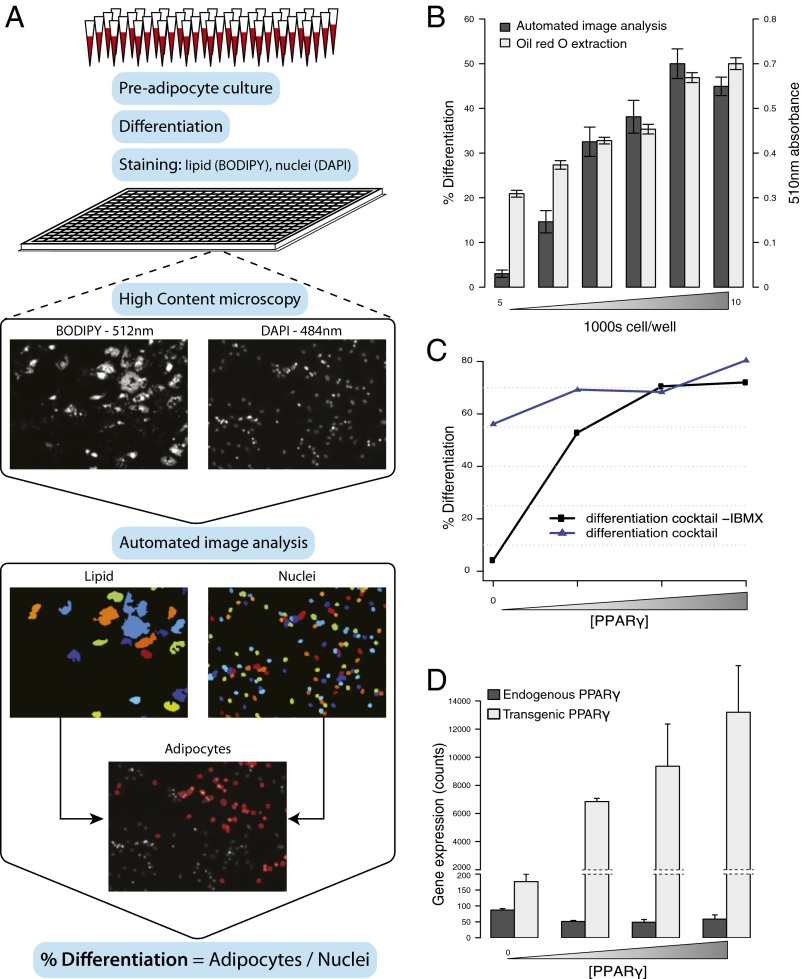
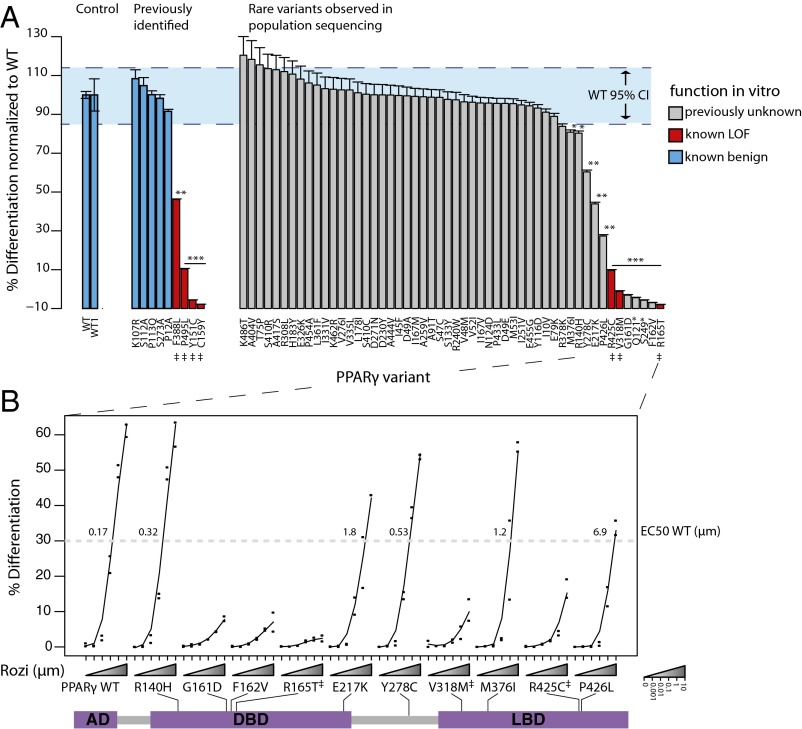
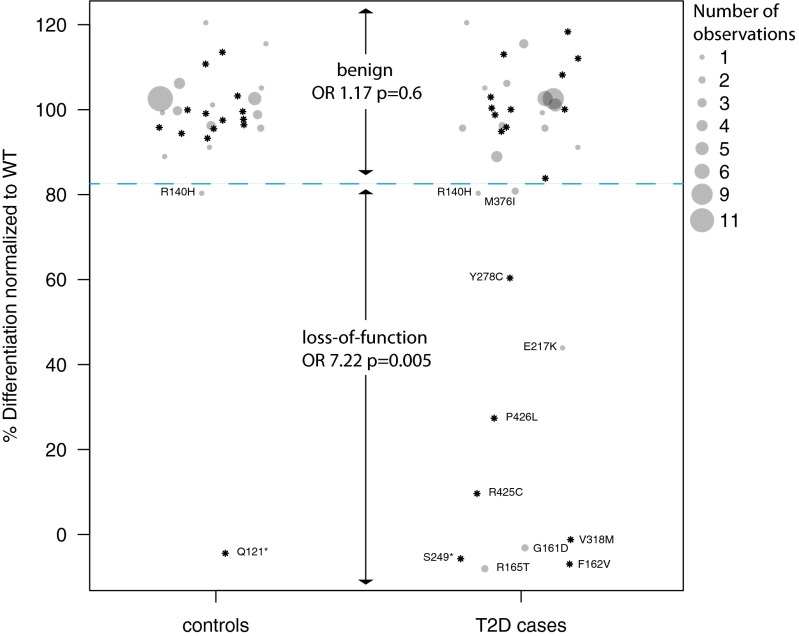
Peroxisome proliferator-activated receptor gamma (PPARG) is a master transcriptional regulator of adipocyte differentiation and a canonical target of antidiabetic thiazolidinedione medications. In rare families, loss-of-function (LOF) mutations in PPARG are known to cosegregate with lipodystrophy and insulin resistance; in the general population, the common P12A variant is associated with a decreased risk of type 2 diabetes (T2D). Whether and how rare variants in PPARG and defects in adipocyte differentiation influence risk of T2D in the general population remains undetermined. By sequencing PPARG in 19,752 T2D cases and controls drawn from multiple studies and ethnic groups, we identified 49 previously unidentified, nonsynonymous PPARG variants (MAF < 0.5%). Considered in aggregate (with or without computational prediction of functional consequence), these rare variants showed no association with T2D (OR = 1.35; P = 0.17). The function of the 49 variants was experimentally tested in a novel high-throughput human adipocyte differentiation assay, and nine were found to have reduced activity in the assay. Carrying any of these nine LOF variants was associated with a substantial increase in risk of T2D (OR = 7.22; P = 0.005). The combination of large-scale DNA sequencing and functional testing in the laboratory reveals that approximately 1 in 1,000 individuals carries a variant in PPARG that reduces function in a human adipocyte differentiation assay and is associated with a substantial risk of T2D.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Deeb SS, et al. A Pro12Ala substitution in PPARgamma2 associated with decreased receptor activity, lower body mass index and improved insulin sensitivity. Nat Genet. 1998;20(3):284–287. - PubMed
-
- Stumvoll M, Häring H. The peroxisome proliferator-activated receptor-γ2 Pro12Ala polymorphism. Diabetes. 2002;51(8):2341–7. - PubMed
-
- Altshuler D, et al. The common PPARgamma Pro12Ala polymorphism is associated with decreased risk of type 2 diabetes. Nat Genet. 2000;26(1):76–80. - PubMed
-
- Barroso I, et al. Dominant negative mutations in human PPARgamma associated with severe insulin resistance, diabetes mellitus and hypertension. Nature. 1999;402(6764):880–883. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 DK085501/DK/NIDDK NIH HHS/United States
- R00 DK092251/DK/NIDDK NIH HHS/United States
- 5U01DK085526/DK/NIDDK NIH HHS/United States
- R01 DK098032/DK/NIDDK NIH HHS/United States
- HHSN268201300049C/HL/NHLBI NIH HHS/United States
- R01 GM089652/GM/NIGMS NIH HHS/United States
- RC2 DK088389/DK/NIDDK NIH HHS/United States
- HHSN268201300046C/HL/NHLBI NIH HHS/United States
- GM089652/GM/NIGMS NIH HHS/United States
- U54 HG003067/HG/NHGRI NIH HHS/United States
- U01 DK085524/DK/NIDDK NIH HHS/United States
- U01 DK085545/DK/NIDDK NIH HHS/United States
- K08 DK102877/DK/NIDDK NIH HHS/United States
- U54HG003067/HG/NHGRI NIH HHS/United States
- HHSN268201300048C/HL/NHLBI NIH HHS/United States
- BB/I02593X/1/BB_/Biotechnology and Biological Sciences Research Council/United Kingdom
- HHSN268201300047C/HL/NHLBI NIH HHS/United States
- U01 DK085526/DK/NIDDK NIH HHS/United States
- HHSN268201300050C/HL/NHLBI NIH HHS/United States
- U01 DK085584/DK/NIDDK NIH HHS/United States
- DK085584/DK/NIDDK NIH HHS/United States
- DK085545/DK/NIDDK NIH HHS/United States
- 098395/WT_/Wellcome Trust/United Kingdom
- R01 HL084553/HL/NHLBI NIH HHS/United States
- DK088389/DK/NIDDK NIH HHS/United States
- U01 DK062370/DK/NIDDK NIH HHS/United States
- DK085501/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
