

Induction therapy does not improve survival for clinical stage T2N0 esophageal cancer
- PMID: 25157773
- PMCID: PMC4145610
- DOI: 10.1097/JTO.0000000000000228
Induction therapy does not improve survival for clinical stage T2N0 esophageal cancer
Abstract
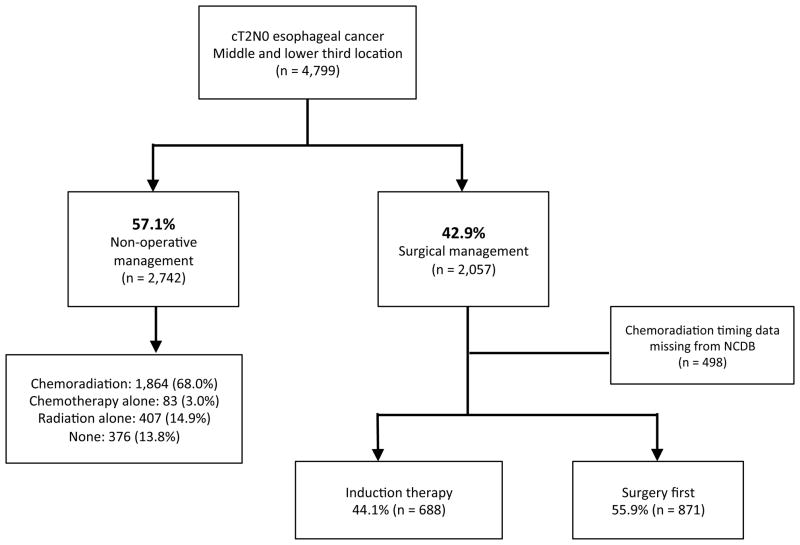
Introduction: This study compared survival after initial treatment with esophagectomy as primary therapy to induction therapy followed by esophagectomy for patients with clinical T2N0 (cT2N0) esophageal cancer in the National Cancer Database (NCDB).
Methods: Predictors of therapy selection for patients with cT2N0 esophageal cancer in the NCDB from 1998 to 2011 were identified with multivariable logistic regression. Survival was evaluated using Kaplan-Meier and Cox proportional hazards methods.
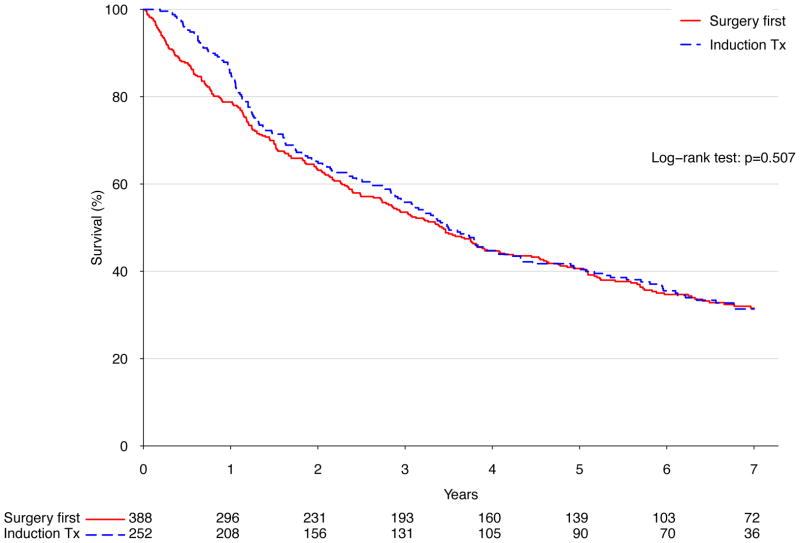
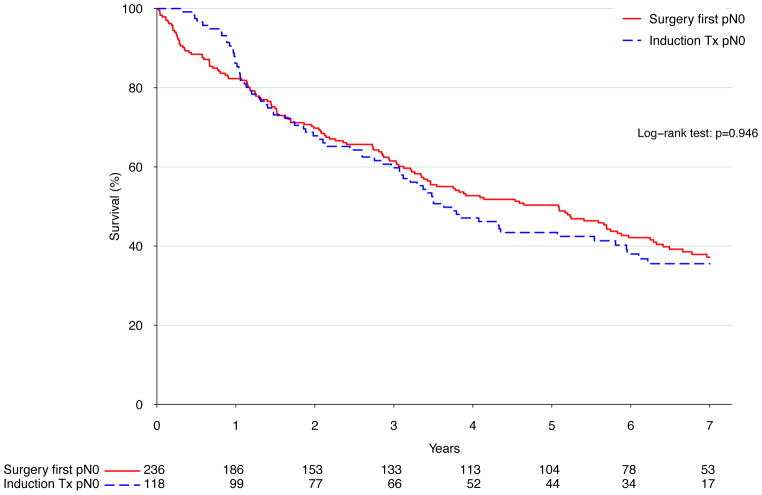
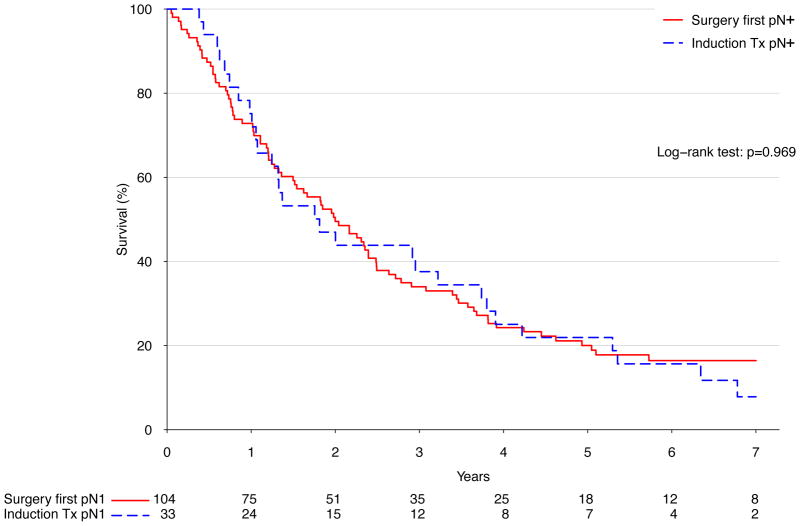
Results: Surgery was used in 42.9% (2057 of 4799) of cT2N0 patients. Of 1599 esophagectomy patients for whom treatment timing was recorded, induction therapy was used in 44.1% (688). Pretreatment staging was proven accurate in only 26.7% of patients (210 of 786) who underwent initial surgery without induction treatment and had complete pathologic data available: 41.6% (n = 327) were upstaged and 31.7% (n = 249) were downstaged. Adjuvant therapy (chemotherapy or radiation therapy) was given to 50.2% of patients treated initially with surgery who were found after resection to have nodal disease. There was no significant difference in long-term survival between strategies of primary surgery and induction therapy followed by surgery (median 41.1 versus 41.9 months, p = 0.51). In multivariable analysis, induction therapy was not independently associated with risk of death (hazard ratio [HR], 1.16, p = 0.32).
Conclusions: Current clinical staging for early-stage esophageal cancer is highly inaccurate, with only a quarter of surgically resected cT2N0 patients found to have had accurate pretreatment staging. Induction therapy for patients with cT2N0 esophageal cancer in the NCDB is not associated with improved survival.
Figures
References
-
- Ajani JA, Barthel JS, Bentrem DJ, et al. Esophageal and esophagogastric junction cancers. Journal of the National Comprehensive Cancer Network: JNCCN. 2011;9:830–887. - PubMed
-
- Crabtree TD, Yacoub WN, Puri V, et al. Endoscopic ultrasound for early stage esophageal adenocarcinoma: implications for staging and survival. The Annals of thoracic surgery. 2011;91:1509–1515. discussion 1515–1506. - PubMed
-
- Rice TW, Mason DP, Murthy SC, et al. T2N0M0 esophageal cancer. The Journal of thoracic and cardiovascular surgery. 2007;133:317–324. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
