

Relationships between Adipose Tissue and Psoriasis, with or without Arthritis
- PMID: 25161652
- PMCID: PMC4129363
- DOI: 10.3389/fimmu.2014.00368
Relationships between Adipose Tissue and Psoriasis, with or without Arthritis
Abstract
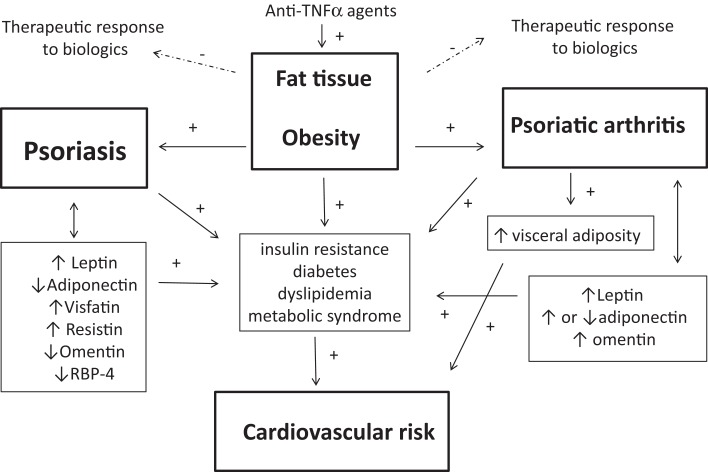
Psoriasis (Pso) is a common chronic cutaneous inflammatory disease involving the skin that is associated with serious comorbidities. Comorbidities in Pso include psoriatic arthritis (PsA), reduced quality of life, malignancy, depression, but also a constellation of associated conditions that enhance the cardiovascular (CV) risk. Indeed, obesity is common in patients with Pso or PsA and is considered to be a risk factor for the onset of these diseases. Patients with Pso and PsA share common obesity-related complications such as metabolic syndrome (MetS), dyslipidemia, diabetes or insulin resistance, and CV diseases. Chronic inflammation in Pso and PsA partially explains the development of atherosclerosis and CV diseases. In parallel, body composition is disturbed in patients with Pso or PsA, as suggested by anthropometric measurements, while an excess of abdominal adiposity is observed in PsA, enhancing the risk of MetS and CV diseases. Adipokines may link the adipose tissue to the obesity-related complications of Pso and PsA. Indeed, altered circulating levels of the adipokines leptin, adiponectin, visfatine, and resistin have been found in patients with Pso or PsA. In addition, an excess of adipose tissue may compromise the therapeutic response to traditional drugs or biological agents in Pso and PsA. This paper reviews the comorbidities that contribute to enhanced CV risk, the body composition results, and the potential role of adipokines in systemic inflammation and energetic balance in Pso and PsA.
Keywords: adipokines; cardiovascular risk; obesity; psoriasis; psoriatic arthritis.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous