

Comparison of clinicopathologic features and survival of histopathologically amelanotic and pigmented melanomas: a population-based study
- PMID: 25162299
- PMCID: PMC4262611
- DOI: 10.1001/jamadermatol.2014.1348
Comparison of clinicopathologic features and survival of histopathologically amelanotic and pigmented melanomas: a population-based study
Abstract
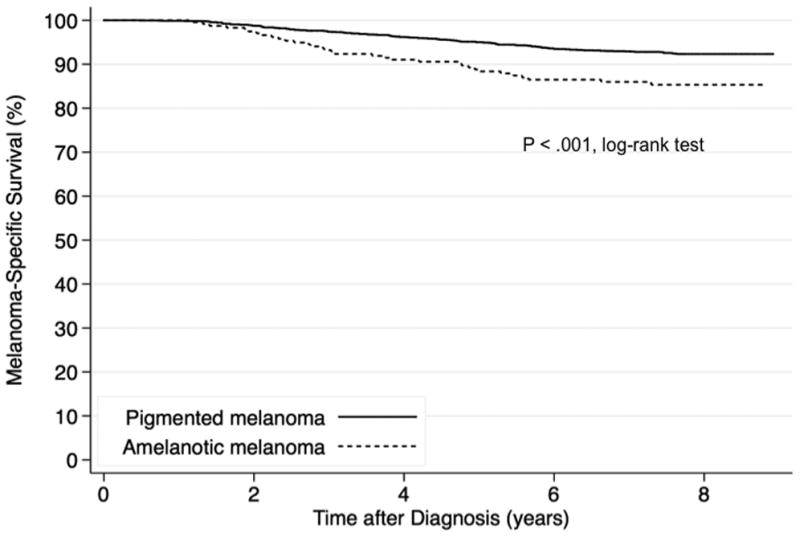
IMPORTANCE Previous studies have reported that histopathologically amelanotic melanoma is associated with poorer survival than pigmented melanoma; however, small numbers of amelanotic melanomas, selected populations, lack of centralized pathologic review, or no adjustment for stage limit the interpretation or generalization of results from prior studies.OBJECTIVE To compare melanoma-specific survival between patients with histopathologically amelanotic and those with pigmented melanoma in a large international population-based study.DESIGN, SETTING, AND PARTICIPANTS Survival analysis with a median follow-up of 7.6 years.The study population comprised 2995 patients with 3486 invasive primary melanomas centrally scored for histologic pigmentation from the Genes, Environment, and Melanoma(GEM) Study, which enrolled incident cases of melanoma diagnosed in 1998 through 2003 from international population-based cancer registries.MAIN OUTCOMES AND MEASURES Clinicopathologic predictors and melanoma-specific survival of histologically amelanotic and pigmented melanoma were compared using generalized estimating equations and Cox regression models, respectively.RESULTS Of 3467 melanomas, 275 (8%) were histopathologically amelanotic. Female sex,nodular and unclassified or other histologic subtypes, increased Breslow thickness, presence of mitoses, severe solar elastosis, and lack of a coexisting nevus were independently associated with amelanotic melanoma (each P < .05). Amelanotic melanoma was generally ofa higher American Joint Committee on Cancer (AJCC) tumor stage at diagnosis (odds ratios[ORs] [95%CIs] between 2.9 [1.8-4.6] and 11.1 [5.8-21.2] for tumor stages between T1b and T3b and ORs [95%CIs] of 24.6 [13.6-44.4] for T4a and 29.1 [15.5-54.9] for T4b relative to T1a;P value for trend, <.001) than pigmented melanoma. Hazard of death from melanoma was higher for amelanotic than for pigmented melanoma (hazard ratio [HR], 2.0; 95%CI, 1.4-3.0)(P < .001), adjusted for age, sex, anatomic site, and study design variables, but survival did not differ once AJCC tumor stage was also taken into account (HR, 0.8; 95%CI, 0.5-1.2)(P = .36).CONCLUSIONS AND RELEVANCE At the population level, survival after diagnosis of amelanotic melanoma is poorer than after pigmented melanoma because of its more advanced stage at diagnosis. It is probable that amelanotic melanomas present at more advanced tumor stages because they are difficult to diagnose. The association of amelanotic melanoma with presence of mitoses independently of Breslow thickness and other clinicopathologic characteristics suggests that amelanotic melanomas might also grow faster than pigmented melanomas. New strategies for early diagnosis and investigation of the biological properties of amelanotic melanoma are warranted.
Conflict of interest statement
Figures
References
-
- Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014 Jan-Feb;64(1):9–29. - PubMed
-
- Hauschild A, Grob JJ, Demidov LV, et al. Dabrafenib in BRAF-mutated metastatic melanoma: a multicentre, open-label, phase 3 randomised controlled trial. Lancet. 2012 Jul 28;380(9839):358–365. - PubMed
-
- Robert C, Flaherty KT, Hersey P, et al. METRIC phase III study: Efficacy of trametinib (T), a potent and selective MEK inhibitor (MEKi), in progression-free survival (PFS) and overall survival (OS) compared with chemotherapy (C) in patients (pts) with BRAFV600/k mutant advanced or metastatic melanoma (MM) J Clin Oncol. 2012;30(15) suppl.
Publication types
MeSH terms
Grants and funding
- P30 ES010126/ES/NIEHS NIH HHS/United States
- R33 CA160138/CA/NCI NIH HHS/United States
- R01 CA112524/CA/NCI NIH HHS/United States
- R01CA112524-05S2/CA/NCI NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- P30 CA014089/CA/NCI NIH HHS/United States
- R01 CA098438/CA/NCI NIH HHS/United States
- R01 CA112243/CA/NCI NIH HHS/United States
- K05 CA131675/CA/NCI NIH HHS/United States
- CA098438/CA/NCI NIH HHS/United States
- R01CA112243-05S1/CA/NCI NIH HHS/United States
- U01CA83180/CA/NCI NIH HHS/United States
- R01CA112243/CA/NCI NIH HHS/United States
- R33CA160138/CA/NCI NIH HHS/United States
- U01 CA083180/CA/NCI NIH HHS/United States
- P30ES010126/ES/NIEHS NIH HHS/United States
- R01CA112524/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
