

Clinical characteristics associated with postoperative intestinal epithelial barrier dysfunction in children with congenital heart disease
- PMID: 25162512
- PMCID: PMC4286428
- DOI: 10.1097/PCC.0000000000000256
Clinical characteristics associated with postoperative intestinal epithelial barrier dysfunction in children with congenital heart disease
Abstract
Objective: Children with congenital heart disease have loss of intestinal epithelial barrier function, which increases their risk for postoperative sepsis and organ dysfunction. We do not understand how postoperative cardiopulmonary support or the inflammatory response to cardiopulmonary bypass might alter intestinal epithelial barrier function. We examined variation in a panel of plasma biomarkers to reflect intestinal epithelial barrier function (cellular and paracellular) after cardiopulmonary bypass and in response to routine ICU care.
Design: Prospective cohort.
Setting: University medical center cardiac ICU.
Patients: Twenty children aged between newborn and 18 years undergoing repair or palliation of congenital heart disease with cardiopulmonary bypass.
Interventions: We measured baseline and repeated plasma intestinal fatty acid-binding protein, citrulline, claudin 3, and dual sugar permeability testing to reflect intestinal epithelial integrity, epithelial function, paracellular integrity, and paracellular function, respectively. We measured baseline and repeated plasma proinflammatory (interleukin-6, tumor necrosis factor-α, and interferon-γ) and anti-inflammatory (interleukin-4 and interleukin-10) cytokines, known to modulate intestinal epithelial barrier function in murine models of cardiopulmonary bypass.
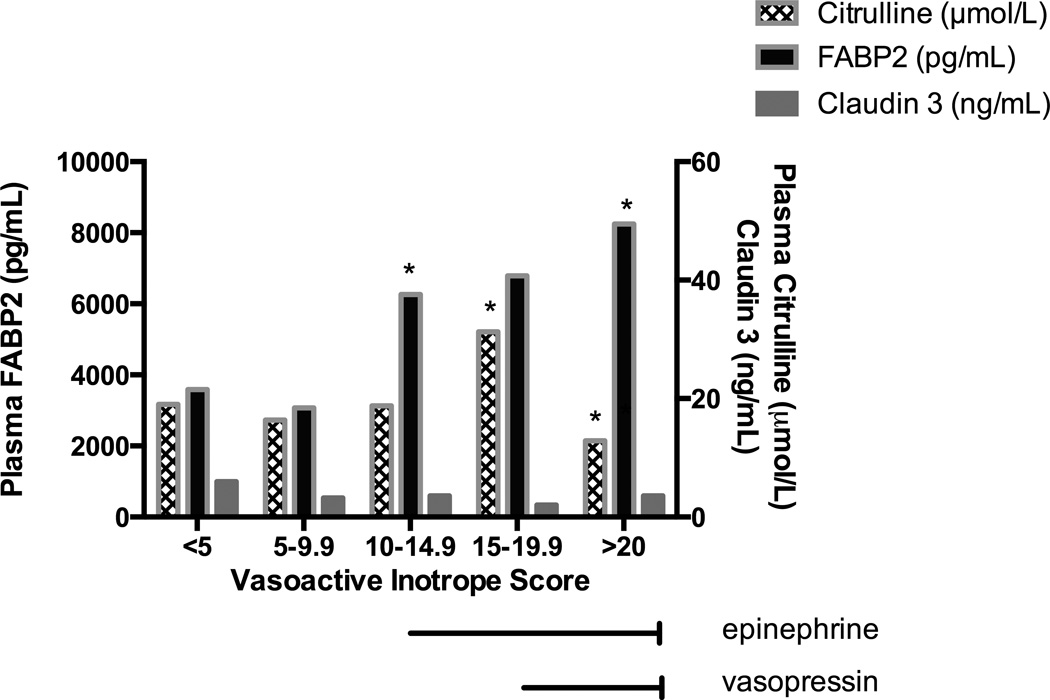
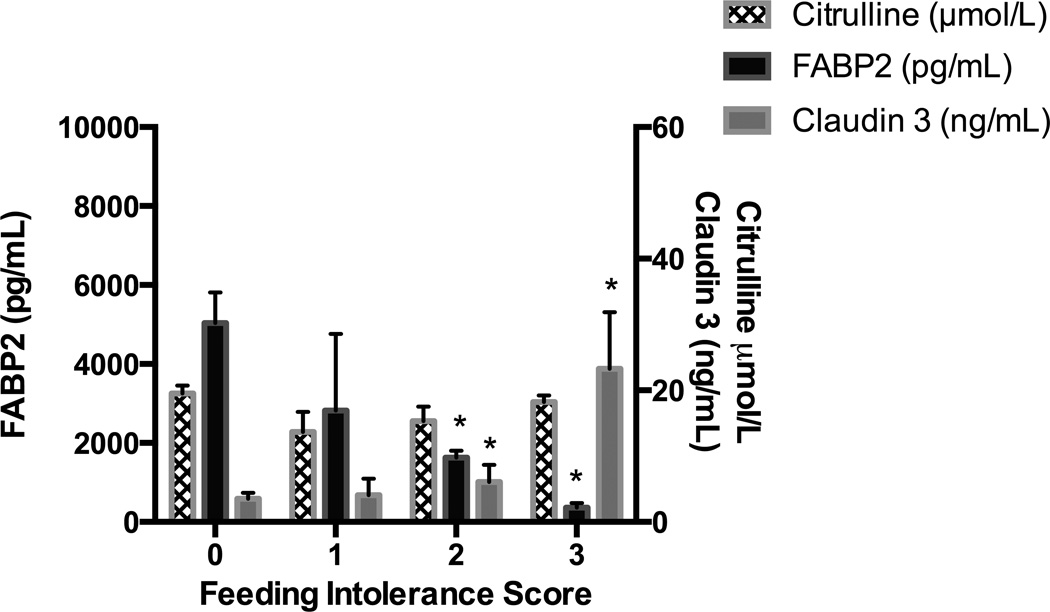
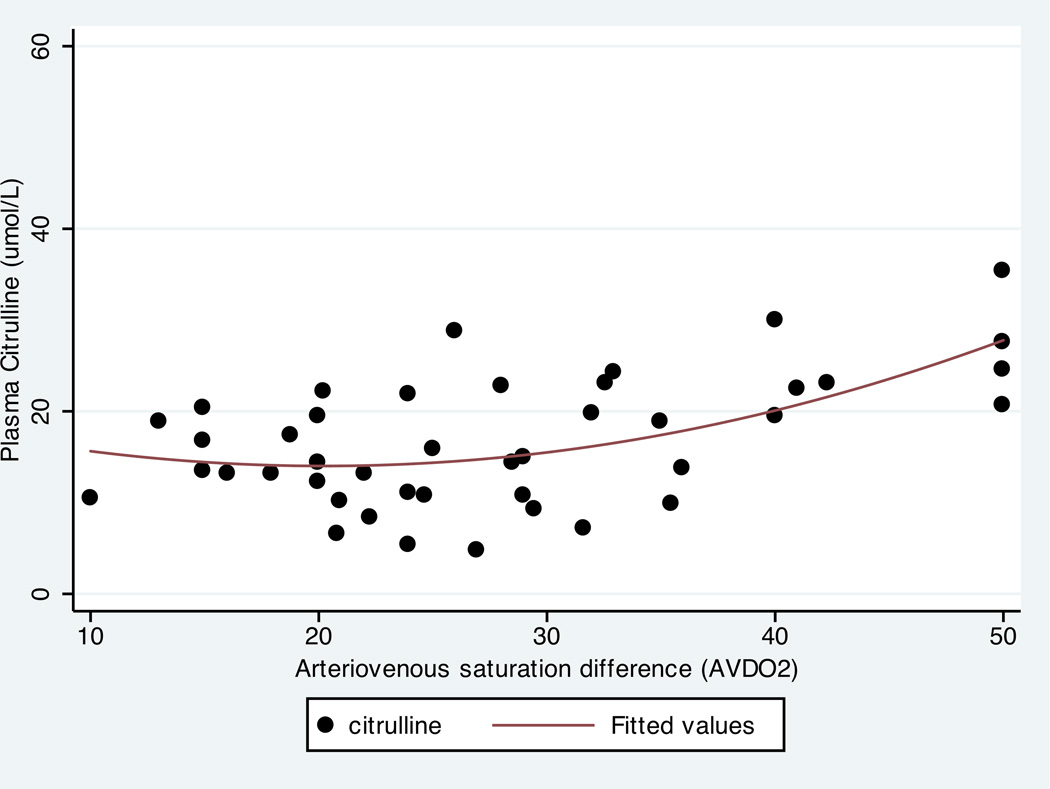
Measurements and main results: All patients had abnormal baseline intestinal fatty acid-binding protein concentrations (mean, 3,815.5 pg/mL; normal, 41-336 pg/mL). Cytokine response to cardiopulmonary bypass was associated with early, but not late, changes in plasma concentrations of intestinal fatty acid-binding protein 2 and citrulline. Variation in biomarker concentrations over time was associated with aspects of ICU care indicating greater severity of illness: claudin 3, intestinal fatty acid-binding protein 2, and dual sugar permeability test ratio were associated with symptoms of feeding intolerance (p < 0.05), whereas intestinal fatty acid-binding protein was positively associated with vasoactive-inotrope score (p = 0.04). Citrulline was associated with larger arteriovenous oxygen saturation difference (p = 0.04) and had a complex relationship with vasoactive-inotrope score.
Conclusions: Children undergoing cardiopulmonary bypass for repair or palliation of congenital heart disease are at risk for intestinal injury and often present with evidence for loss of intestinal epithelial integrity preoperatively. Greater severity of illness requiring increased cardiopulmonary support rather than the inflammatory response to cardiopulmonary bypass seems to mediate late postoperative intestinal epithelial barrier function.
Figures

Comment in
-
Pediatric cardiac surgery with cardiopulmonary bypass: a punch in the gut?Pediatr Crit Care Med. 2015 Jan;16(1):80-1. doi: 10.1097/PCC.0000000000000282. Pediatr Crit Care Med. 2015. PMID: 25560284 No abstract available.
References
-
- Pathan N, Burmester M, Adamovic T, et al. Intestinal injury and endotoxemia in children undergoing surgery for congenital heart disease. American journal of respiratory and critical care medicine. 2011;184:1261–1269. - PubMed
-
- Wildhaber BE, Yang H, Spencer AU, Drongowski RA, Teitelbaum DH. Lack of enteral nutrition--effects on the intestinal immune system. JSurgRes. 2005;123:8–16. - PubMed
-
- Sacks GS, Kudsk KA. Maintaining mucosal immunity during parenteral feeding with surrogates to enteral nutrition. NutrClinPract. 2003;18:483–488. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
