

Pediatric severe sepsis in U.S. children's hospitals
- PMID: 25162514
- PMCID: PMC4221502
- DOI: 10.1097/PCC.0000000000000225
Pediatric severe sepsis in U.S. children's hospitals
Abstract
Objectives: To compare the prevalence, resource utilization, and mortality for pediatric severe sepsis identified using two established identification strategies.
Design: Observational cohort study from 2004 to 2012.
Setting: Forty-four pediatric hospitals contributing data to the Pediatric Health Information Systems database.
Patients: Children 18 years old or younger.
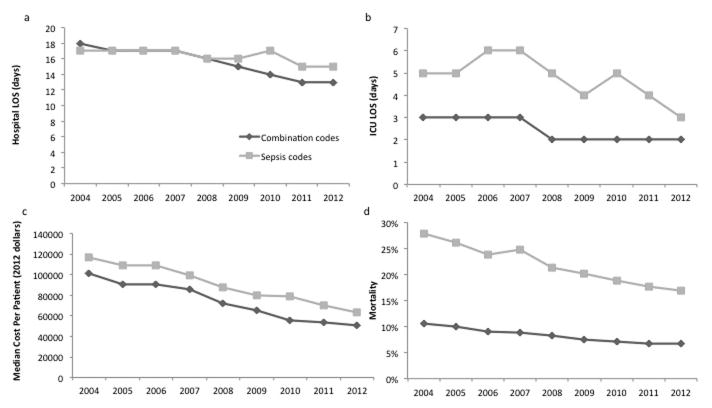
Measurements and main results: We identified patients with severe sepsis or septic shock by using two International Classification of Diseases, 9th edition, Clinical Modification-based coding strategies: 1) combinations of International Classification of Diseases, 9th edition, Clinical Modification codes for infection plus organ dysfunction (combination code cohort); 2) International Classification of Diseases, 9th edition, Clinical Modification codes for severe sepsis and septic shock (sepsis code cohort). Outcomes included prevalence of severe sepsis, as well as hospital and ICU length of stay, and mortality. Outcomes were compared between the two cohorts examining aggregate differences over the study period and trends over time. The combination code cohort identified 176,124 hospitalizations (3.1% of all hospitalizations), whereas the sepsis code cohort identified 25,236 hospitalizations (0.45%), a seven-fold difference. Between 2004 and 2012, the prevalence of sepsis increased from 3.7% to 4.4% using the combination code cohort and from 0.4% to 0.7% using the sepsis code cohort (p < 0.001 for trend in each cohort). Length of stay (hospital and ICU) and costs decreased in both cohorts over the study period (p < 0.001). Overall, hospital mortality was higher in the sepsis code cohort than the combination code cohort (21.2% [95% CI, 20.7-21.8] vs 8.2% [95% CI, 8.0-8.3]). Over the 9-year study period, there was an absolute reduction in mortality of 10.9% (p < 0.001) in the sepsis code cohort and 3.8% (p < 0.001) in the combination code cohort.
Conclusions: Prevalence of pediatric severe sepsis increased in the studied U.S. children's hospitals over the past 9 years, whereas resource utilization and mortality decreased. Epidemiologic estimates of pediatric severe sepsis varied up to seven-fold depending on the strategy used for case ascertainment.
Figures

Comment in
-
Sepsis or SEPSIS: does it make a difference?Pediatr Crit Care Med. 2014 Nov;15(9):893-4. doi: 10.1097/PCC.0000000000000259. Pediatr Crit Care Med. 2014. PMID: 25370053 No abstract available.
-
Sepsis Is SEPSIS! It's High Time to Globalize Pediatric Sepsis.Pediatr Crit Care Med. 2015 May;16(4):390-1. doi: 10.1097/PCC.0000000000000376. Pediatr Crit Care Med. 2015. PMID: 25946271 No abstract available.
-
The authors reply.Pediatr Crit Care Med. 2015 May;16(4):392-3. doi: 10.1097/PCC.0000000000000394. Pediatr Crit Care Med. 2015. PMID: 25946273 Free PMC article. No abstract available.
References
-
- National Vital Statistics System, Natioanl Center for Health Statistics, Centers for Disease Control and Prevention. 2010
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29:1303–1310. - PubMed
-
- Marshall JC. Sepsis: rethinking the approach to clinical research. J Leukoc Biol. 2008;83:471–482. - PubMed
-
- Geroulanos S, Douka ET. Historical perspective of the word “sepsis”. Intensive Care Med. 2006;32:2077. - PubMed
-
- Levy MM, Fink MP, Marshall JC, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Intensive Care Med. 2003;29:530–538. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
