

Self-management support interventions to reduce health care utilisation without compromising outcomes: a systematic review and meta-analysis
- PMID: 25164529
- PMCID: PMC4177163
- DOI: 10.1186/1472-6963-14-356
Self-management support interventions to reduce health care utilisation without compromising outcomes: a systematic review and meta-analysis
Abstract
Background: There is increasing interest in the role of 'self-management' interventions to support the management of long-term conditions in health service settings. Self-management may include patient education, support for decision-making, self-monitoring and psychological and social support. Self-management support has potential to improve the efficiency of health services by reducing other forms of utilisation (such as primary care or hospital use), but a shift to self-management may lead to negative outcomes, such as patients who feel more anxious about their health, are less able to cope, or who receive worse quality of care, all of which may impact on their health and quality of life. We sought to determine which models of self-management support are associated with significant reductions in health services utilisation without compromising outcomes among patients with long-term conditions.
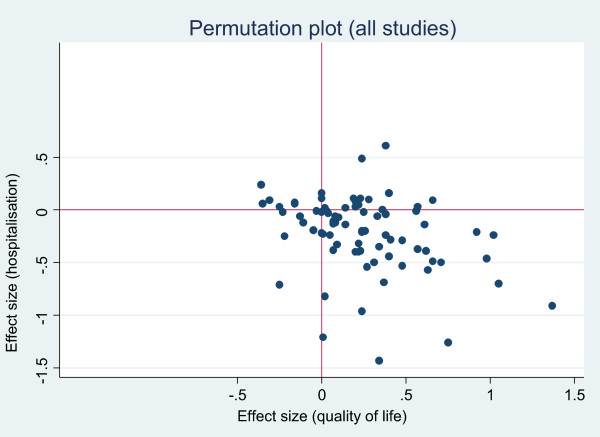
Methods: We used systematic review with meta-analysis. We included randomised controlled trials in patients with long-term conditions which included self-management support interventions and reported measures of service utilisation or costs, as well as measures of health outcomes (standardized disease specific quality of life, generic quality of life, or depression/anxiety).We searched multiple databases (CENTRAL, CINAHL, Econlit, EMBASE, HEED, MEDLINE, NHS EED and PsycINFO) and the reference lists of published reviews. We calculated effects sizes for both outcomes and costs, and presented the results in permutation plots, as well as conventional meta-analyses.
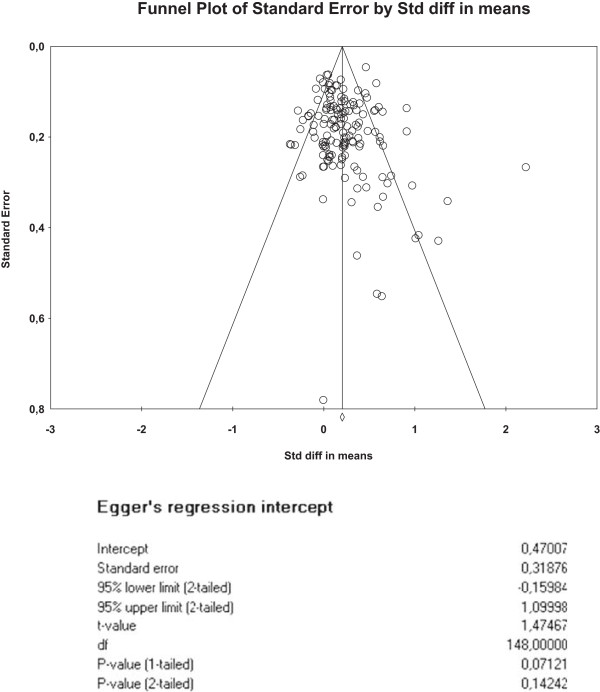
Results: We included 184 studies. Self-management support was associated with small but significant improvements in health outcomes, with the best evidence of effectiveness in patients with diabetic, respiratory, cardiovascular and mental health conditions. Only a minority of self-management support interventions reported reductions in health care utilisation in association with decrements in health. Evidence for reductions in utilisation associated with self-management support was strongest in respiratory and cardiovascular problems. Studies at higher risk of bias were more likely to report benefits.
Conclusions: Self-management support interventions can reduce health service utilization without compromising patient health outcomes, although effects were generally small, and the evidence was strongest in respiratory and cardiovascular disorders. Further work is needed to determine which components of self-management support are most effective.
Figures




References
-
- Murray C, Lopez A. The global burden of disease: a comprehensive assessment of mortality and disability from disease, injuries and risk factors in 1990. Boston: Harvard University Press; 1996.
Pre-publication history
-
- The pre-publication history for this paper can be accessed here: http://www.biomedcentral.com/1472-6963/14/356/prepub
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
