

Renal replacement therapy for autosomal dominant polycystic kidney disease (ADPKD) in Europe: prevalence and survival--an analysis of data from the ERA-EDTA Registry
- PMID: 25165182
- PMCID: PMC7611099
- DOI: 10.1093/ndt/gfu017
Renal replacement therapy for autosomal dominant polycystic kidney disease (ADPKD) in Europe: prevalence and survival--an analysis of data from the ERA-EDTA Registry
Abstract
Background: Autosomal dominant polycystic kidney disease (ADPKD) is the fourth most common renal disease requiring renal replacement therapy (RRT). Still, there are few epidemiological data on the prevalence of, and survival on RRT for ADPKD.
Methods: This study used data from the ERA-EDTA Registry on RRT prevalence and survival on RRT in 12 European countries with 208 million inhabitants. We studied four 5-year periods (1991-2010). Survival analysis was performed by the Kaplan-Meier method and by Cox proportional hazards regression.
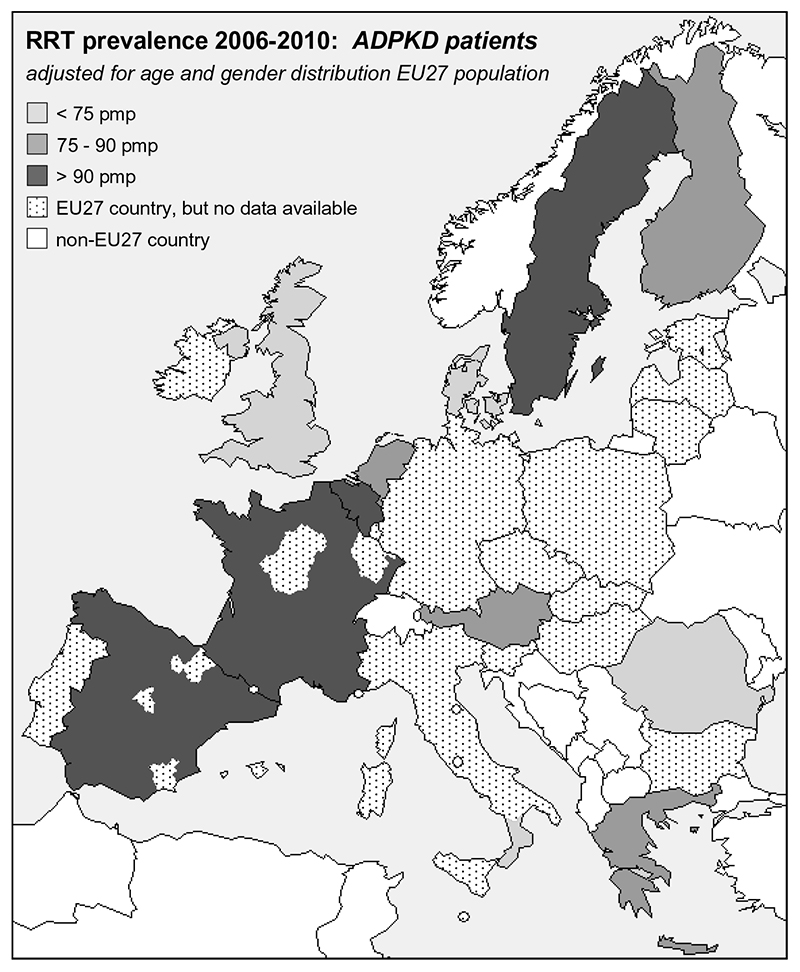
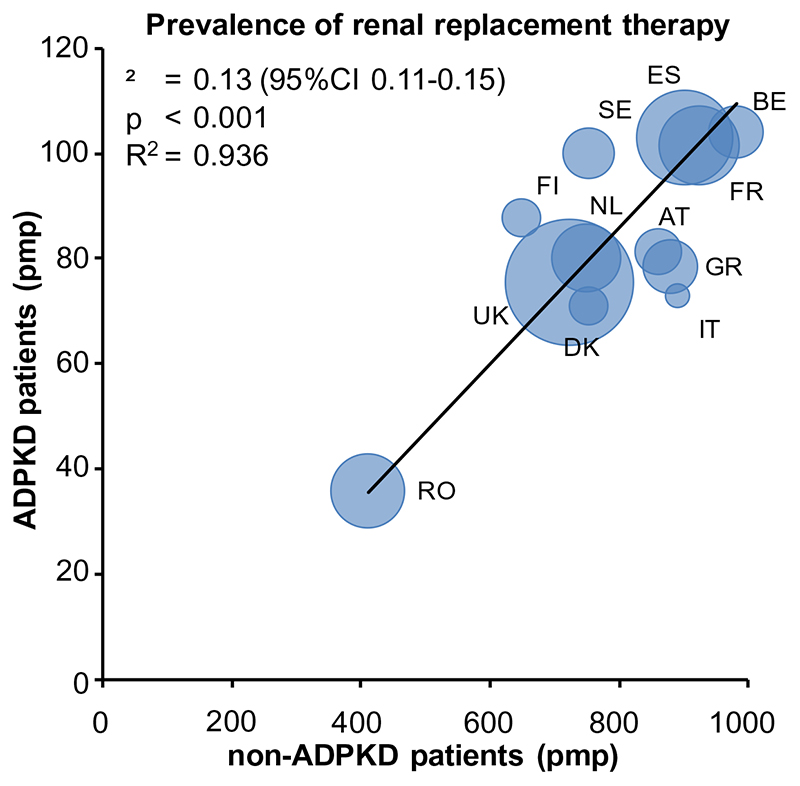
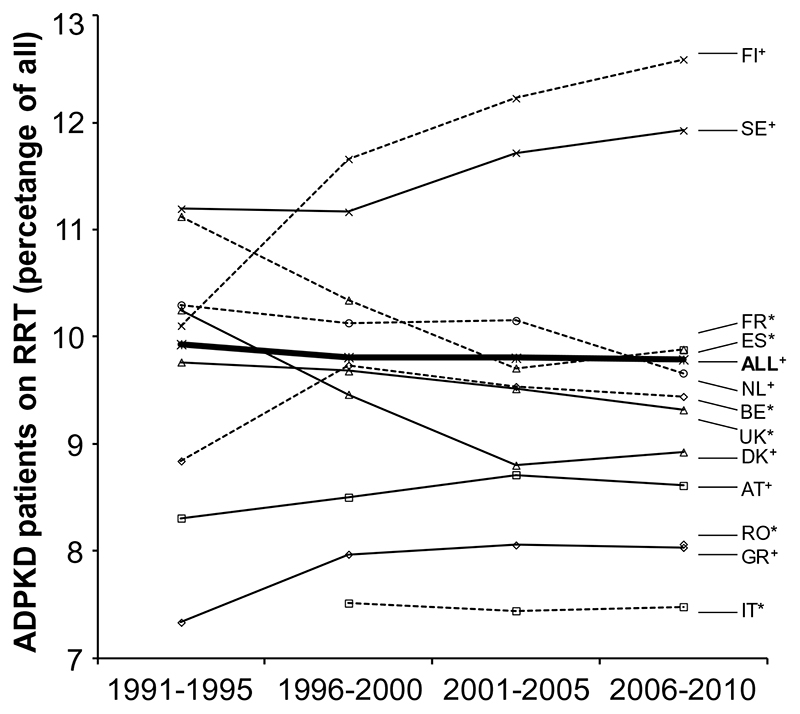
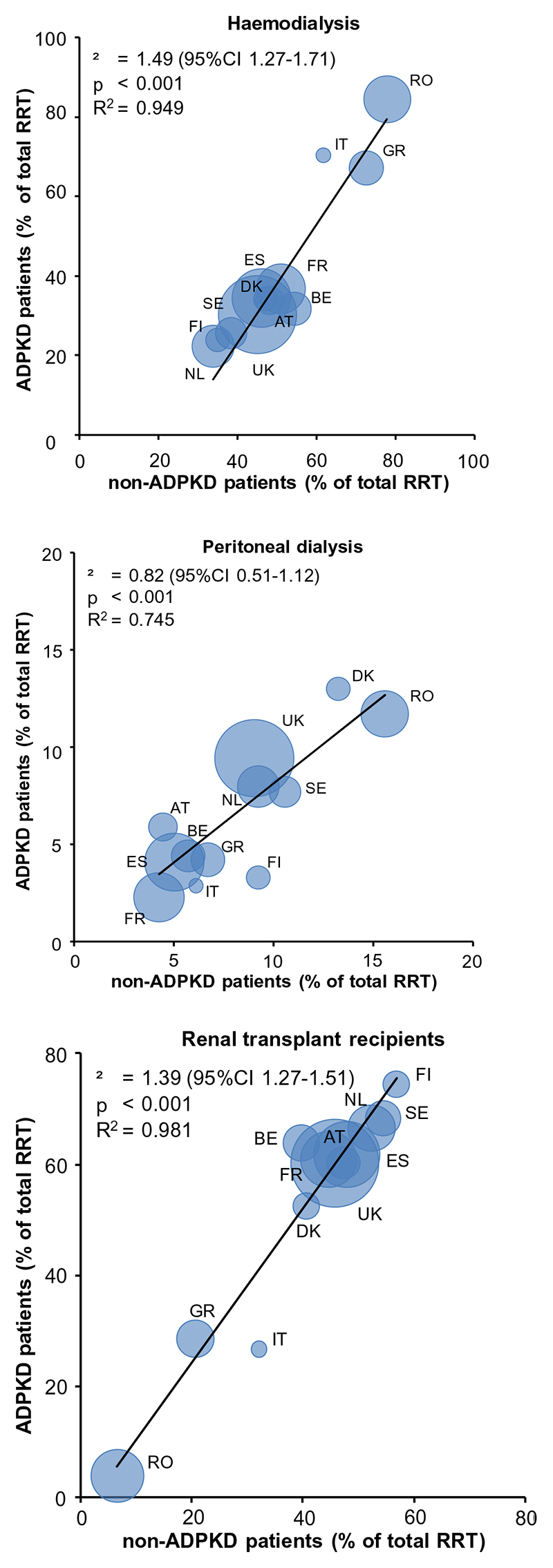
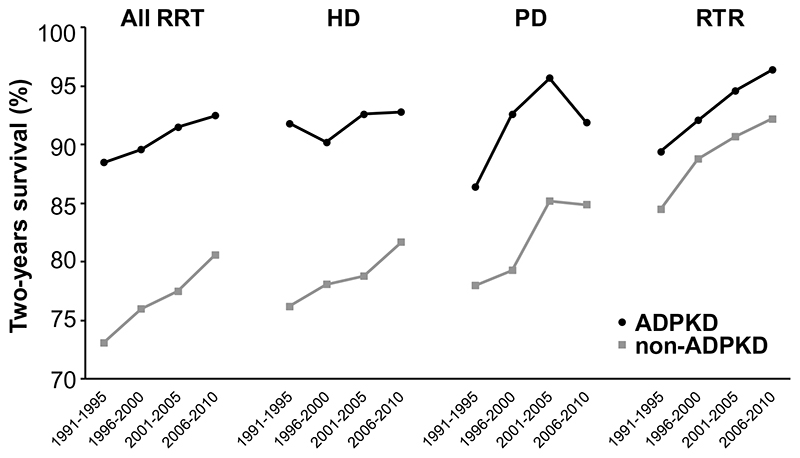
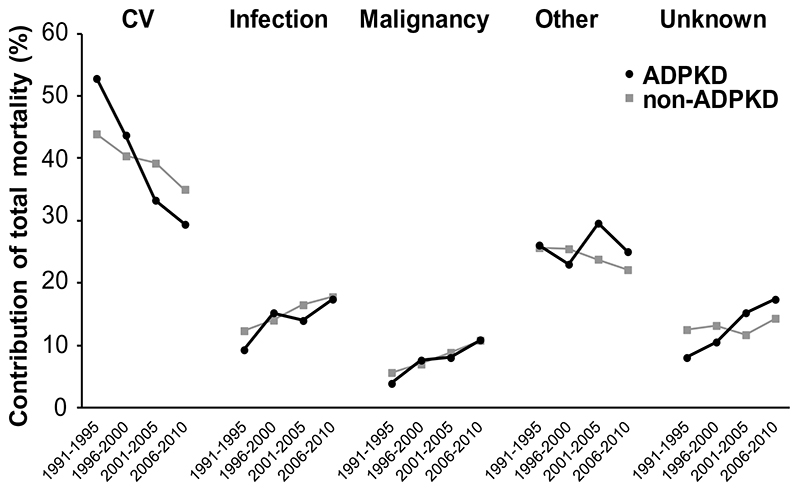
Results: From the first to the last study period, the prevalence of RRT for ADPKD increased from 56.8 to 91.1 per million population (pmp). The percentage of prevalent RRT patients with ADPKD remained fairly stable at 9.8%. Two-year survival of ADPKD patients on RRT (adjusted for age, sex and country) increased significantly from 89.0 to 92.8%, and was higher than for non-ADPKD subjects. Improved survival was noted for all RRT modalities: haemodialysis [adjusted hazard ratio for mortality during the last versus first time period 0.75 (95% confidence interval 0.61-0.91), peritoneal dialysis 0.55 (0.38-0.80) and transplantation 0.52 (0.32-0.74)]. Cardiovascular mortality as a proportion of total mortality on RRT decreased more in ADPKD patients (from 53 to 29%), than in non-ADPKD patients (from 44 to 35%). Of note, the incidence rate of RRT for ADPKD remained relatively stable at 7.6 versus 8.3 pmp from the first to the last study period, which will be discussed in detail in a separate study.
Conclusions: In ADPKD patients on RRT, survival has improved markedly, especially due to a decrease in cardiovascular mortality. This has led to a considerable increase in the number of ADPKD patients being treated with RRT.
Keywords: ADPKD; epidemiology; prevalence; renal replacement therapy; survival.
© The Author 2014. Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved.
Conflict of interest statement
All authors declare that the results presented in this paper have not been published previously in whole or part, except in abstract format. None to declare is applicable for all the authors.
Figures
References
-
- Torres VE, Harris PC, Pirson Y. Autosomal dominant polycystic kidney disease. Lancet. 2007;369:1287–1301. - PubMed
-
- Hateboer N, v Dijk MA, Bogdanova N, et al. Comparison of phenotypes of polycystic kidney disease types 1 and 2. European PKD1-PKD2 Study Group. Lancet. 1999;353:103–107. - PubMed
-
- Iglesias CG, Torres VE, Offord KP, Holley KE, Beard CM, Kurland LT. Epidemiology of adult polycystic kidney disease, Olmsted County, Minnesota: 1935-1980. AmJKidney Dis. 1983;2:630–639. - PubMed
-
- Gabow PA. Autosomal dominant polycystic kidney disease. N Engl J Med. 1993;329:332–342. - PubMed
-
- Grantham JJ. Clinical practice. Autosomal dominant polycystic kidney disease. N Engl J Med. 2008;359:1477–1485. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
