

Repair of segmental load-bearing bone defect by autologous mesenchymal stem cells and plasma-derived fibrin impregnated ceramic block results in early recovery of limb function
- PMID: 25165699
- PMCID: PMC4109366
- DOI: 10.1155/2014/345910
Repair of segmental load-bearing bone defect by autologous mesenchymal stem cells and plasma-derived fibrin impregnated ceramic block results in early recovery of limb function
Abstract
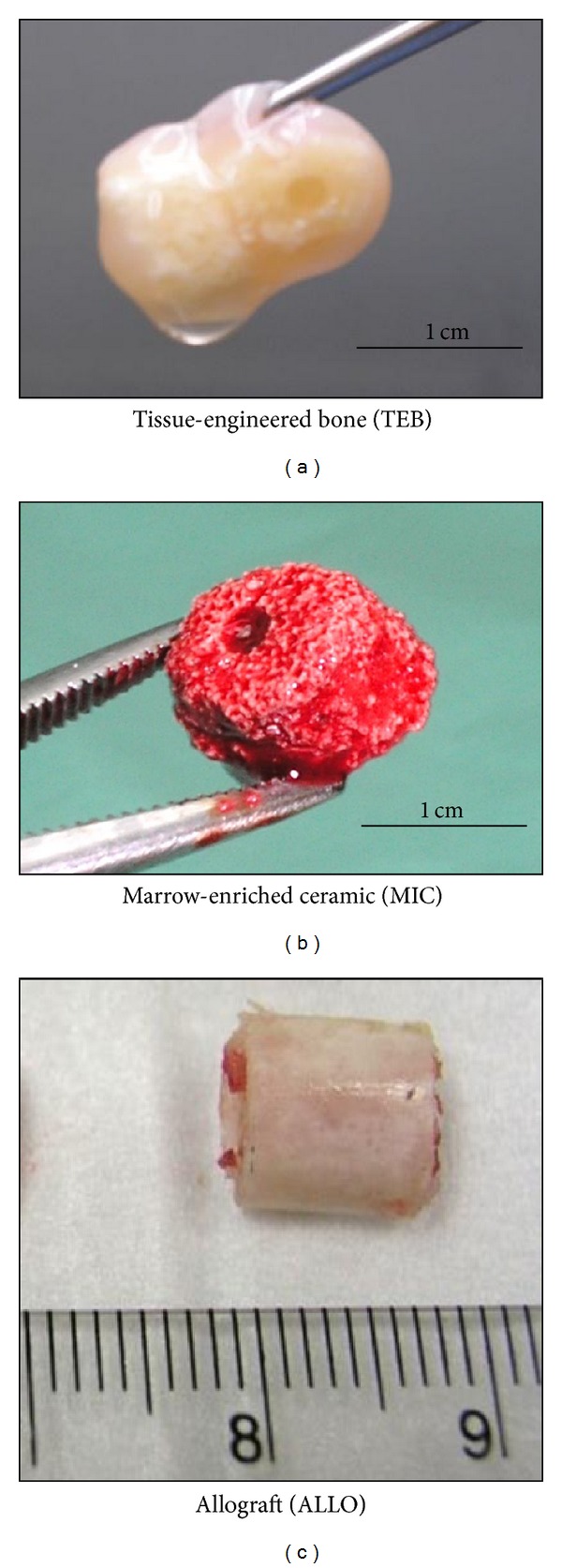
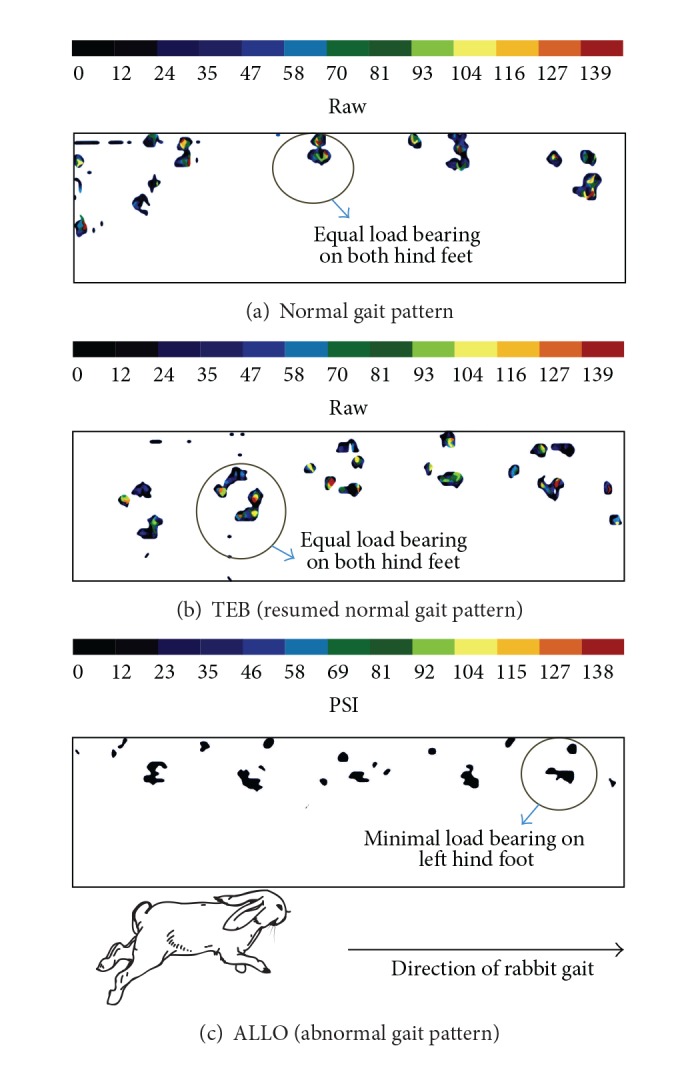
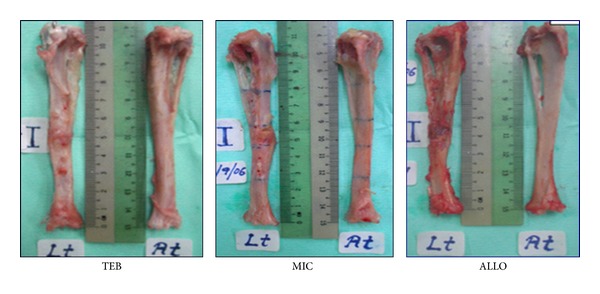
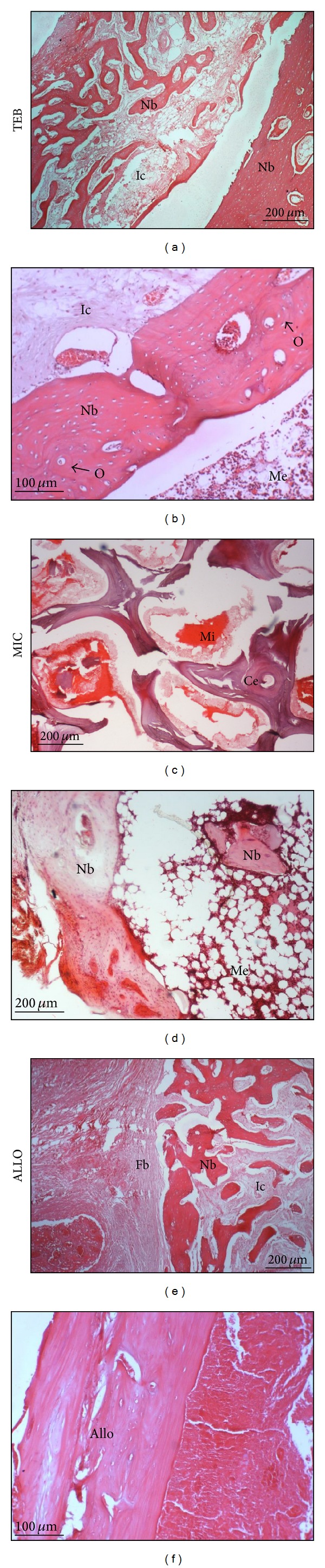
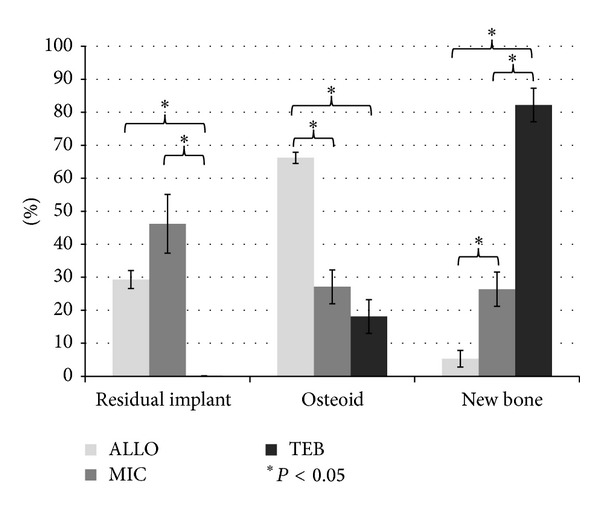
Calcium phosphate-based bone substitutes have not been used to repair load-bearing bone defects due to their weak mechanical property. In this study, we reevaluated the functional outcomes of combining ceramic block with osteogenic-induced mesenchymal stem cells and platelet-rich plasma (TEB) to repair critical-sized segmental tibial defect. Comparisons were made with fresh marrow-impregnated ceramic block (MIC) and partially demineralized allogeneic bone block (ALLO). Six New Zealand White female rabbits were used in each study group and three rabbits with no implants were used as negative controls. By Day 90, 4/6 rabbits in TEB group and 2/6 in ALLO and MIC groups resumed normal gait pattern. Union was achieved significantly faster in TEB group with a radiological score of 4.50 ± 0.78 versus ALLO (1.06 ± 0.32), MIC (1.28 ± 0.24), and negative controls (0). Histologically, TEB group scored the highest percentage of new bone (82% ± 5.1%) compared to ALLO (5% ± 2.5%) and MIC (26% ± 5.2%). Biomechanically, TEB-treated tibiae achieved the highest compressive strength (43.50 ± 12.72 MPa) compared to those treated with ALLO (15.15 ± 3.57 MPa) and MIC (23.28 ± 6.14 MPa). In conclusion, TEB can repair critical-sized segmental load-bearing bone defects and restore limb function.
Figures

References
-
- Rodriguez-Merchan EC, Forriol F. Nonunion: general principles experimental data. Clinical Orthopaedics and Related Research. 2004;419:4–12. - PubMed
-
- Sulaiman AR, Nordin S, Faisham WI, Zulmi W, Halim AS. Residual nonunion following vascularised fibular graft treatment for congenital pseudarthrosis of the tibia: a report of two cases. Journal of Orthopaedic Surgery. 2006;14(1):64–66. - PubMed
-
- Paley D, Maar DC. Ilizarov bone transport treatment for tibial defects. Journal of Orthopaedic Trauma. 2000;14(2):76–85. - PubMed
-
- Jannetty J, Kolb E, Boxberger J, Deslauriers R, Ganey T. Guiding bone formation in a critical-sized defect and assessments. Journal of Craniofacial Surgery. 2010;21(6):1848–1854. - PubMed
-
- Rose REC. Pin site care with the Ilizarov circular fixator. Internet Journal of Orthopaedic Surgery. 2010;16(1)
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
