

Pulmonary hypertension and right heart dysfunction in chronic lung disease
- PMID: 25165714
- PMCID: PMC4140123
- DOI: 10.1155/2014/739674
Pulmonary hypertension and right heart dysfunction in chronic lung disease
Abstract
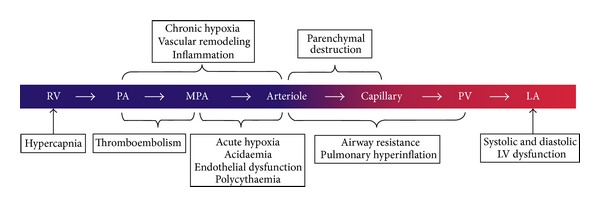
Group 3 pulmonary hypertension (PH) is a common complication of chronic lung disease (CLD), including chronic obstructive pulmonary disease (COPD), interstitial lung disease, and sleep-disordered breathing. Development of PH is associated with poor prognosis and may progress to right heart failure, however, in the majority of the patients with CLD, PH is mild to moderate and only a small number of patients develop severe PH. The pathophysiology of PH in CLD is multifactorial and includes hypoxic pulmonary vasoconstriction, pulmonary vascular remodeling, small vessel destruction, and fibrosis. The effects of PH on the right ventricle (RV) range between early RV remodeling, hypertrophy, dilatation, and eventual failure with associated increased mortality. The golden standard for diagnosis of PH is right heart catheterization, however, evidence of PH can be appreciated on clinical examination, serology, radiological imaging, and Doppler echocardiography. Treatment of PH in CLD focuses on management of the underlying lung disorder and hypoxia. There is, however, limited evidence to suggest that PH-specific vasodilators such as phosphodiesterase-type 5 inhibitors, endothelin receptor antagonists, and prostanoids may have a role in the treatment of patients with CLD and moderate-to-severe PH.
Figures



References
-
- Simonneau G, Robbins IM, Beghetti M, et al. Updated clinical classification of pulmonary hypertension. Journal of the American College of Cardiology. 2013;62(25, supplement):D34–D41. - PubMed
-
- Freixa X, Portillo K, Paré C, et al. Echocardiographic abnormalities in patients with COPD at their first hospital admission. European Respiratory Journal. 2013;41(4):784–791. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
