

The calcineurin inhibitor tacrolimus reduces proteinuria in membranous nephropathy accompanied by a decrease in angiopoietin-like-4
- PMID: 25165975
- PMCID: PMC4148427
- DOI: 10.1371/journal.pone.0106164
The calcineurin inhibitor tacrolimus reduces proteinuria in membranous nephropathy accompanied by a decrease in angiopoietin-like-4
Abstract
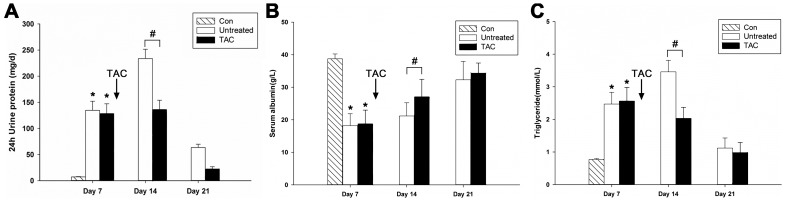
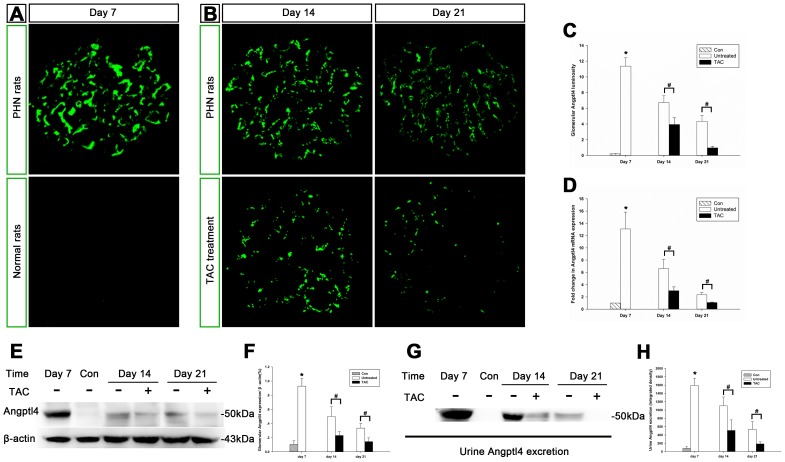
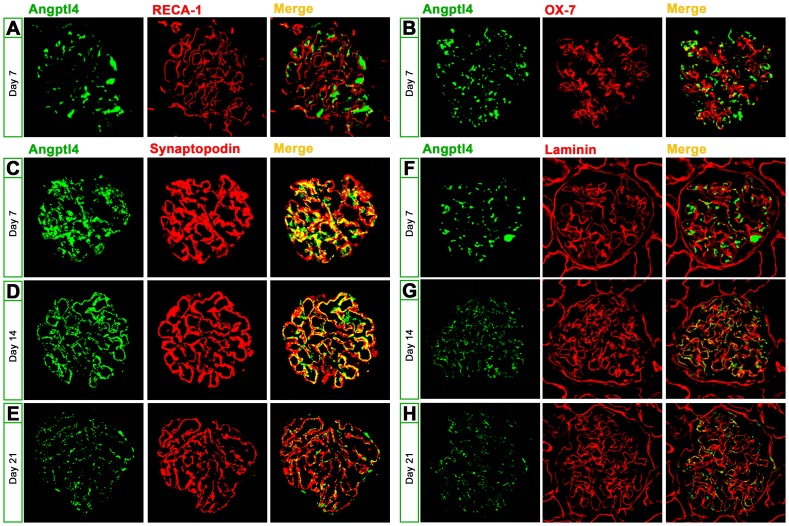
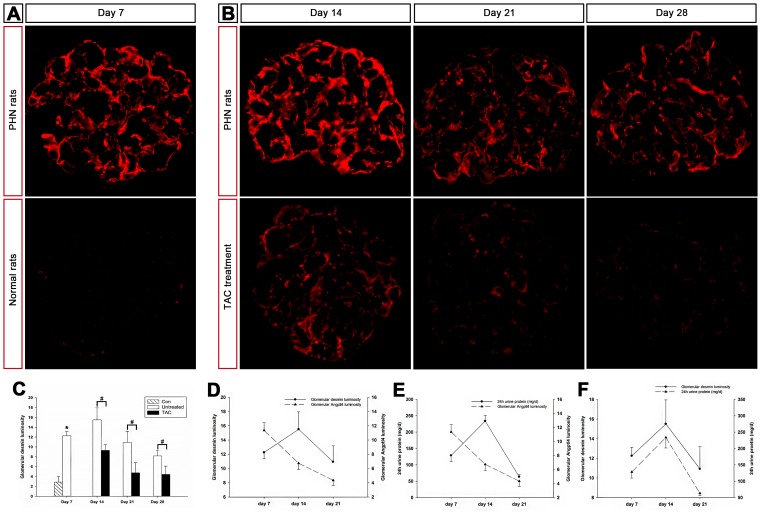
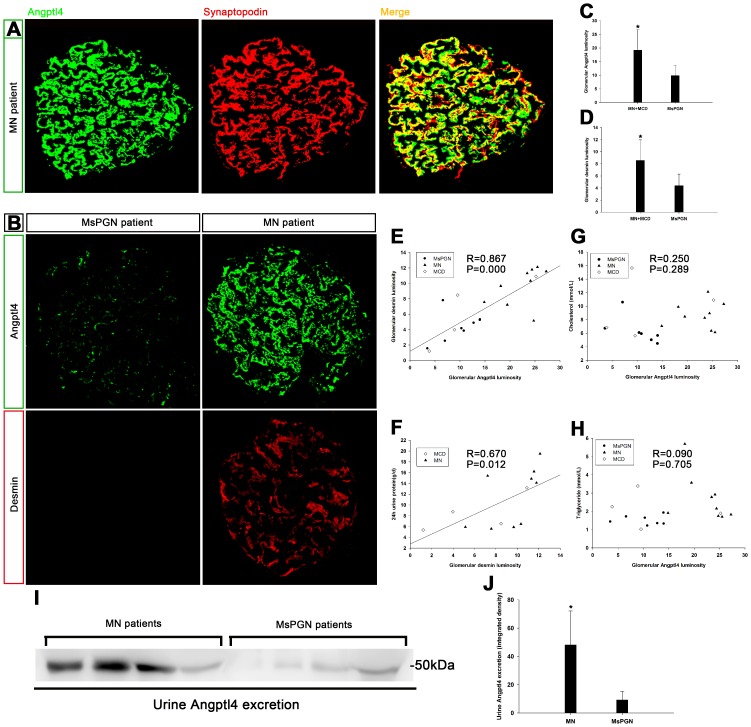
Tacrolimus is an anticalcineurinic agent with potent immunosuppressive activity that has recently been shown to have the added benefit of reducing proteinuria in membranous nephropathy (MN) patients. However, its potential mechanisms remain unknown. To reveal the mechanism, rat cohorts were administered tacrolimus or vehicle from days 7 to 28 after the induction of passive Heymann nephritis (PHN). PHN induction resulted in heavy proteinuria and increased expression of desmin, a marker of injured podocytes. We also showed that the glomerular expression of angiopoietin-like-4 (Angptl4) was markedly upregulated in PHN rats and human MN followed by an increase in urine Angptl4 excretion. In addition, increased Angptl4 expression may be related to podocyte injury and proteinuria. Furthermore, upregulated Angptl4 expression primarily colocalized with podocytes rather than endothelial or mesangial cells, indicating that podocytes may be the source of Angptl4, which then gradually migrated to the glomerular basement membrane over time. However, tacrolimus treatment markedly reduced glomerular and urinary Angptl4, accompanied by a reduction in the established proteinuria and the promotion of podocyte repair. Additionally, glomerular immune deposits and circulating IgG levels induced by PHN clearly decreased following tacrolimus treatment. In conclusion, this is the first demonstration that the calcineurin inhibitor tacrolimus can reduce Angptl4 in podocytes accompanied by a decrease in established proteinuria and promotion of podocyte repair in MN.
Conflict of interest statement
Figures

References
-
- Li LS, Liu ZH (2004) Epidemiologic data of renal diseases from a single unit in China: analysis based on 13,519 renal biopsies. Kidney Int 66: 920–923. - PubMed
-
- Naumovic R, Pavlovic S, Stojkovic D, Basta-Jovanovic G, Nesic V (2009) Renal biopsy registry from a single centre in Serbia: 20 years of experience. Nephrol Dial Transplant 24: 877–885. - PubMed
-
- Ronco P, Debiec H (2012) Pathogenesis of membranous nephropathy: recent advances and future challenges. Nat Rev Nephrol 8: 203–213. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
