

Antibiotic management of lung infections in cystic fibrosis. II. Nontuberculous mycobacteria, anaerobic bacteria, and fungi
- PMID: 25167882
- PMCID: PMC5469357
- DOI: 10.1513/AnnalsATS.201405-203AS
Antibiotic management of lung infections in cystic fibrosis. II. Nontuberculous mycobacteria, anaerobic bacteria, and fungi
Abstract
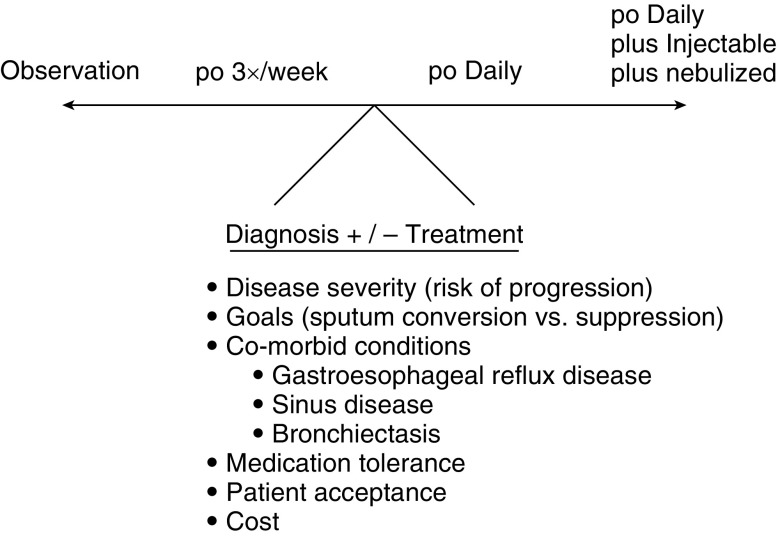
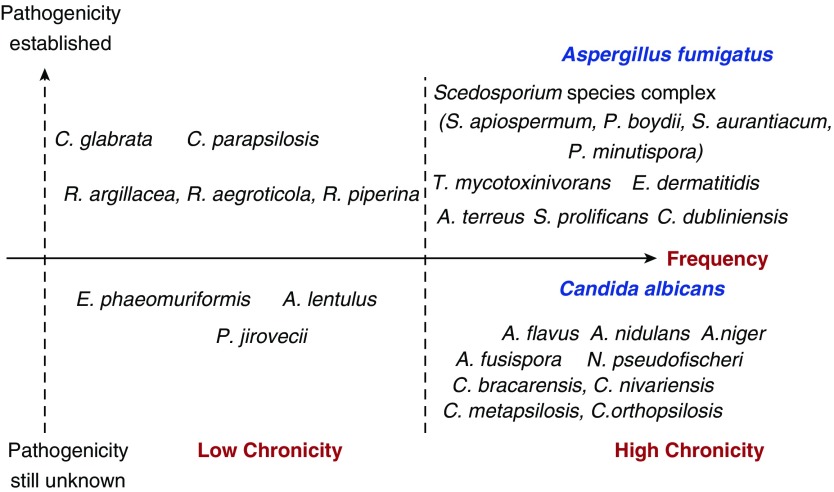
Airway infections are a key component of cystic fibrosis (CF) lung disease. Whereas the approach to common pathogens such as Pseudomonas aeruginosa is guided by a significant body of evidence, other infections often pose a considerable challenge to treating physicians. In Part I of this series on the antibiotic management of difficult lung infections, we discussed bacterial organisms including methicillin-resistant Staphylococcus aureus, gram-negative bacterial infections, and treatment of multiple bacterial pathogens. Here, we summarize the approach to infections with nontuberculous mycobacteria, anaerobic bacteria, and fungi. Nontuberculous mycobacteria can significantly impact the course of lung disease in patients with CF, but differentiation between colonization and infection is difficult clinically as coinfection with other micro-organisms is common. Treatment consists of different classes of antibiotics, varies in intensity, and is best guided by a team of specialized clinicians and microbiologists. The ability of anaerobic bacteria to contribute to CF lung disease is less clear, even though clinical relevance has been reported in individual patients. Anaerobes detected in CF sputum are often resistant to multiple drugs, and treatment has not yet been shown to positively affect patient outcome. Fungi have gained significant interest as potential CF pathogens. Although the role of Candida is largely unclear, there is mounting evidence that Scedosporium species and Aspergillus fumigatus, beyond the classical presentation of allergic bronchopulmonary aspergillosis, can be relevant in patients with CF and treatment should be considered. At present, however there remains limited information on how best to select patients who could benefit from antifungal therapy.
Keywords: Aspergillus fumigatus; Mycobacterium abscessus; Mycobacterium avium complex; Scedosporium species complex; anaerobic bacteria.
Figures
References
-
- Davis PB. Cystic fibrosis since 1938. Am J Respir Crit Care Med. 2006;173:475–482. - PubMed
-
- Courtney JM, Dunbar KE, McDowell A, Moore JE, Warke TJ, Stevenson M, Elborn JS. Clinical outcome of Burkholderia cepacia complex infection in cystic fibrosis adults. J Cyst Fibros. 2004;3:93–98. - PubMed
-
- Dasenbrook EC, Merlo CA, Diener-West M, Lechtzin N, Boyle MP. Persistent methicillin-resistant Staphylococcus aureus and rate of FEV1 decline in cystic fibrosis. Am J Respir Crit Care Med. 2008;178:814–821. - PubMed
-
- Demko CA, Byard PJ, Davis PB. Gender differences in cystic fibrosis: Pseudomonas aeruginosa infection. J Clin Epidemiol. 1995;48:1041–1049. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
