

Do Physicians' Financial Incentives Affect Medical Treatment and Patient Health?
- PMID: 25170174
- PMCID: PMC4144420
- DOI: 10.1257/aer.104.4.1320
Do Physicians' Financial Incentives Affect Medical Treatment and Patient Health?
Abstract
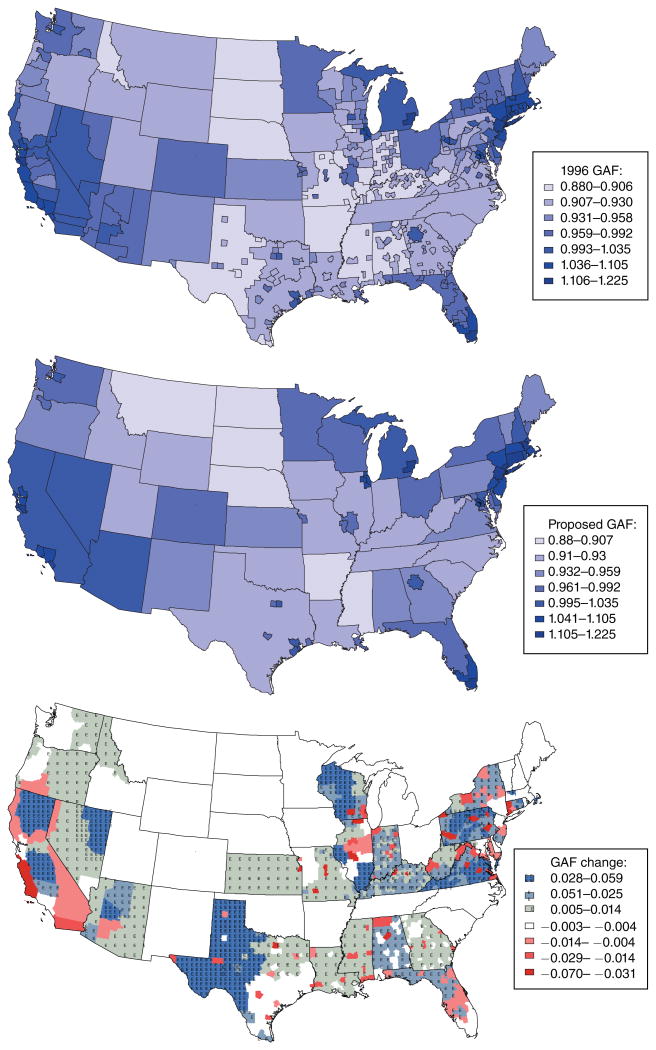
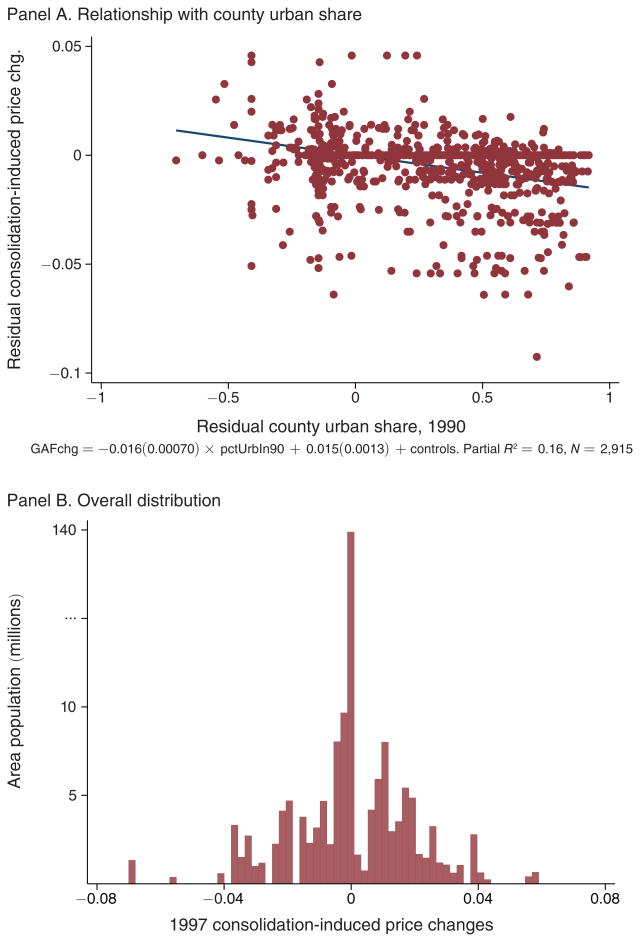
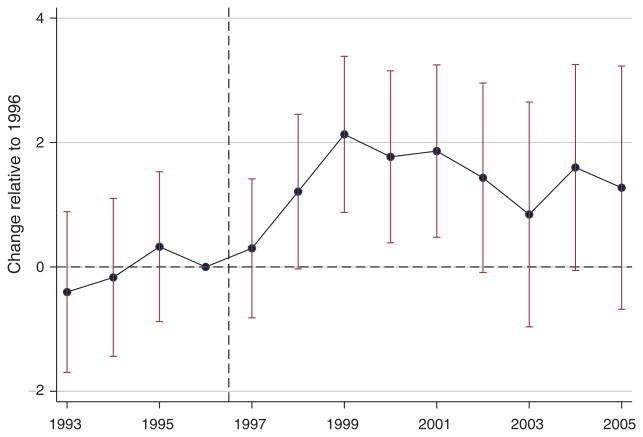
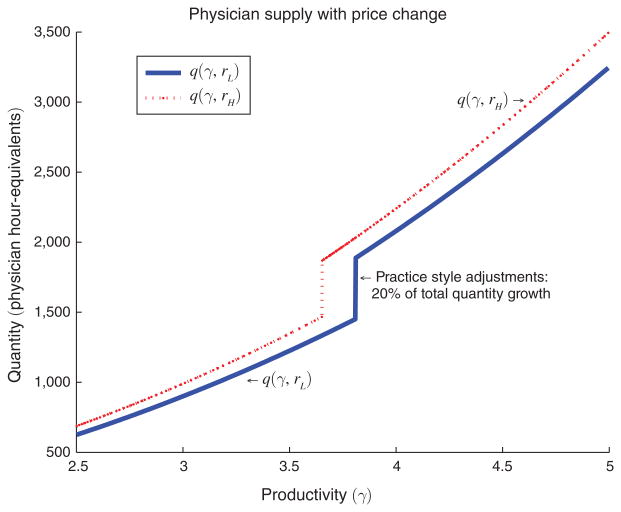
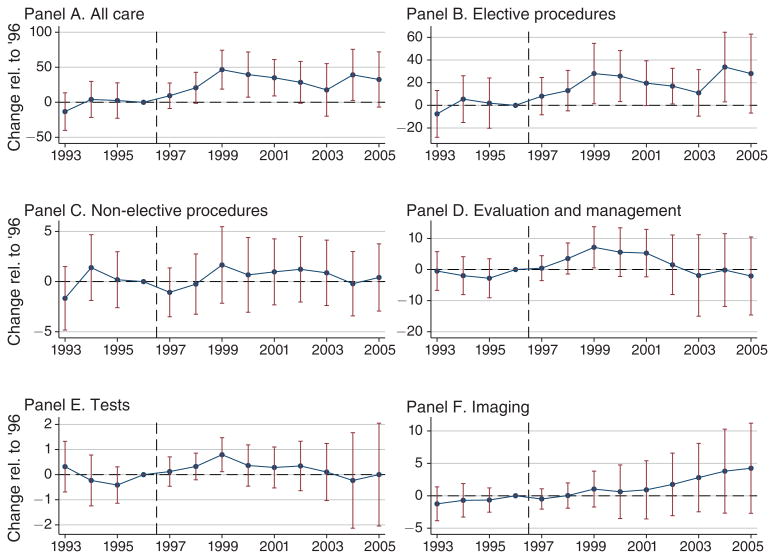
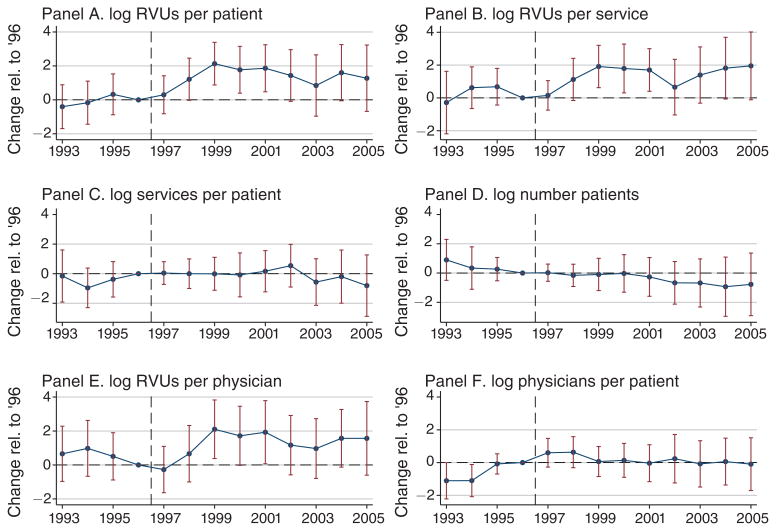
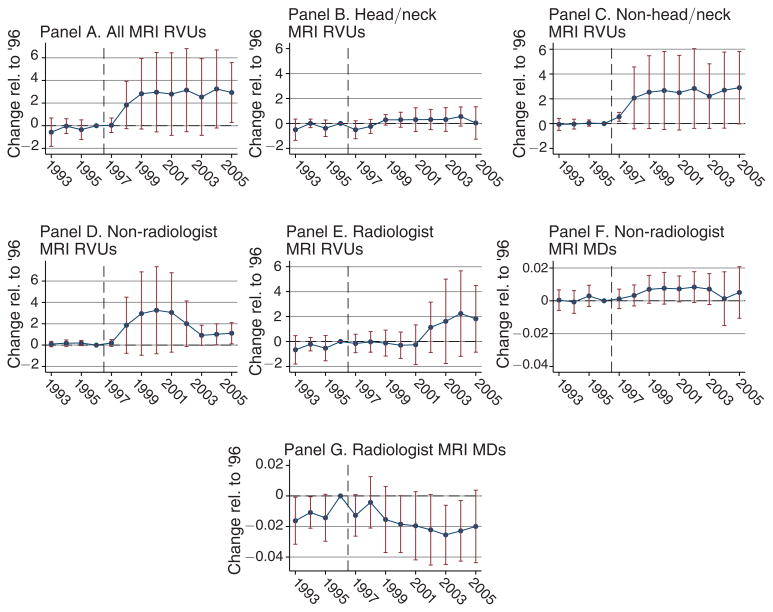
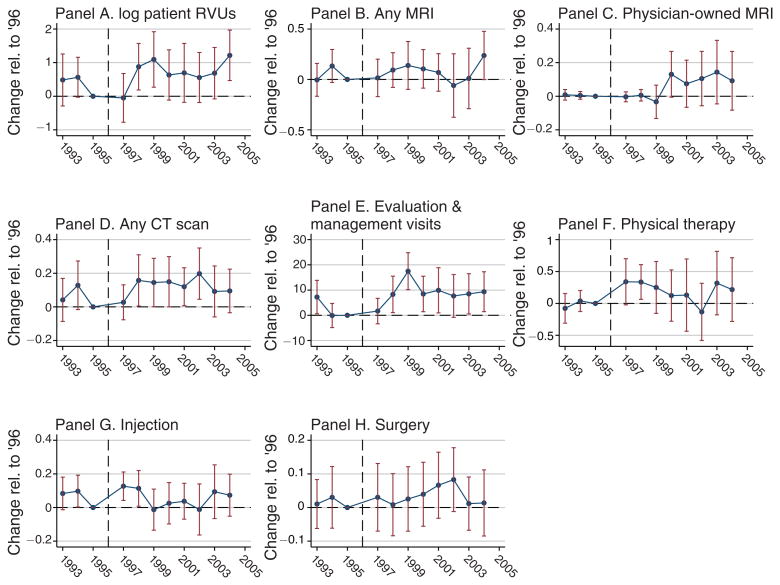
We investigate whether physicians' financial incentives influence health care supply, technology diffusion, and resulting patient outcomes. In 1997, Medicare consolidated the geographic regions across which it adjusts physician payments, generating area-specific price shocks. Areas with higher payment shocks experience significant increases in health care supply. On average, a 2 percent increase in payment rates leads to a 3 percent increase in care provision. Elective procedures such as cataract surgery respond much more strongly than less discretionary services. Non-radiologists expand their provision of MRIs, suggesting effects on technology adoption. We estimate economically small health impacts, albeit with limited precision.
Figures
References
-
- Acemoglu Daron, Finkelstein Amy. Input and Technology Choices in Regulated Industries: Evidence from the Health Care Sector. Journal of Political Economy. 2008;116(5):837–80.
-
- Acemoglu Daron, Linn Joshua. Market Size in Innovation: Theory and Evidence from the Pharmaceutical Industry. Quarterly Journal of Economics. 2004;119(3):1049–90.
-
- Arrow Kenneth J. Uncertainty and the Welfare Economics of Medical Care. American Economic Review. 1963;53(5):941–73.
-
- Arrow KennethJ, Auerbach Alan, Bertko John, Shannon Brownlee, Casalino LawrenceP, Cooper Jim, Crosson FrancisJ, et al. Toward a 21st-Century Health Care System: Recommendations for Health Care Reform. Annals of Internal Medicine. 2009;150(7):493–95. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical