

Review
doi: 10.2147/VHRM.S46452.
eCollection 2014.
Thoracoabdominal aortic aneurysm repair: current endovascular perspectives
Affiliations
- PMID: 25170271
- PMCID: PMC4145733
- DOI: 10.2147/VHRM.S46452
Item in Clipboard
Review
Thoracoabdominal aortic aneurysm repair: current endovascular perspectives
Vasc Health Risk Manag.
.
Abstract
Thoracoabdominal aneurysms account for roughly 3% of identified aneurysms annually in the United States. Advancements in endovascular techniques and devices have broadened their application to these complex surgical problems. This paper will focus on the current state of endovascular thoracoabdominal aneurysm repair, including specific considerations in patient selection, operative planning, and perioperative complications. Both total endovascular and hybrid options will be considered.
Keywords: TEVAR; endovascular surgery; thoracic aorta; thoracoabdominal aneurysm.
Figures
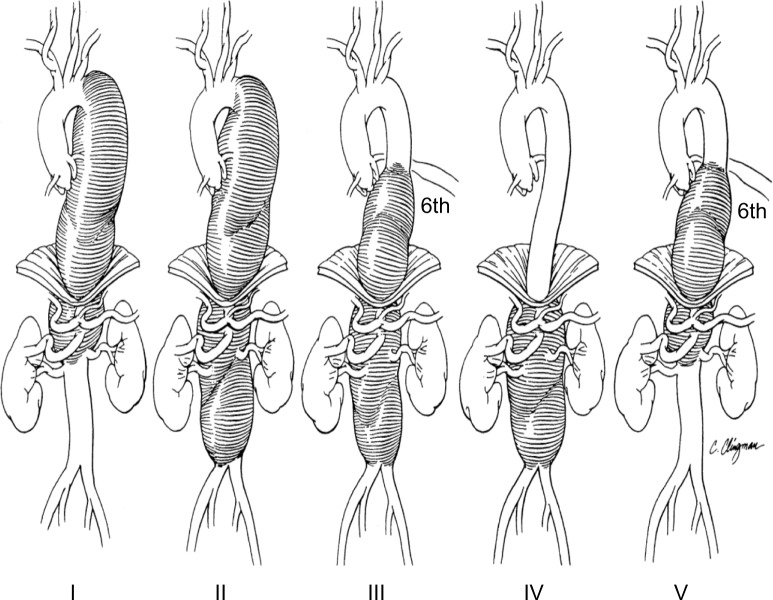
Thoracoabdominal aneurysm classification. Notes: Type I extends from the left subclavian artery to the celiac axis. Type II extends from the left subclavian artery and includes the infrarenal abdominal aorta to the level of the aortic bifurcation. Type III extends from the sixth intercostal space to the iliac bifurcation. Type IV extends from the visceral abdominal aorta to the iliac bifurcation. Type V extends from the sixth intercostal space to just above the renal arteries. Reprinted from The Annals of Thoracic Surgery, 67(6), Safi HJ, Miller CC 3rd, Spinal cord protection in descending thoracic and thoracoabdominal aortic repair, 1937–1939, Copyright © 1999, with permission from Elsevier.
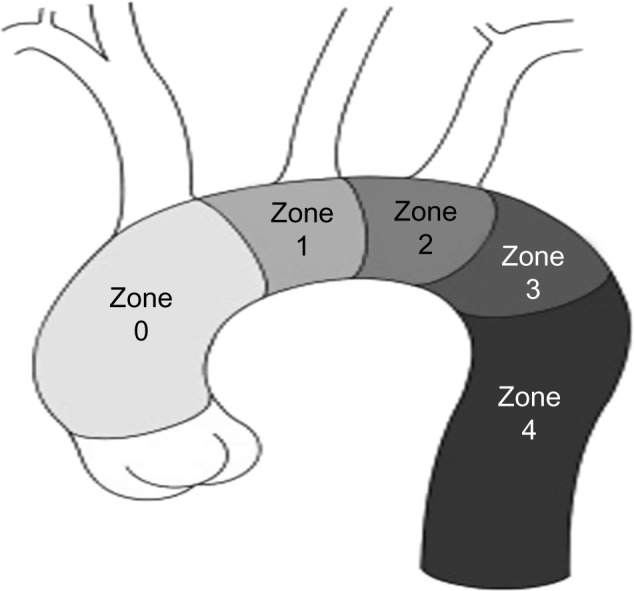
Zones of the aortic arch. Notes: Proximal landing zone attachment sites for endovascular graft deployment. Reprinted from Surg Clin North Am, 89(4), Adams JD, Garcia LM, Kern JA, Endovascular repair of the thoracic aorta, 895–912, Copyright © 2009, with permission from Elsevier.
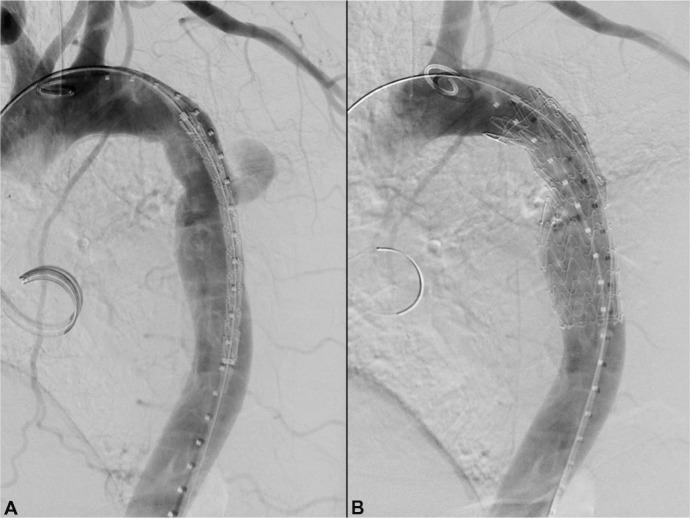
Salvage TEVAR. Notes: Salvage of failing prior open aortic transection repair using standard TEVAR technique. This 62-year-old patient had had a previous open aortic transection repair at the age of 18 years after a motor vehicle crash. Nearly 45 years later, he presented with acute onset left sided chest and back pain. On CTA he was found to have a pseudoaneurysmal contained leak at his previous anastomotic suture line (A). A single TEVAR device was deployed to cover the suture line pseudoaneurysm (B). His pain resolved and is event free 2 years later. Abbreviations: TEVAR, thoracic endovascular aneurysm repair; CTA, computed tomographic angiography.
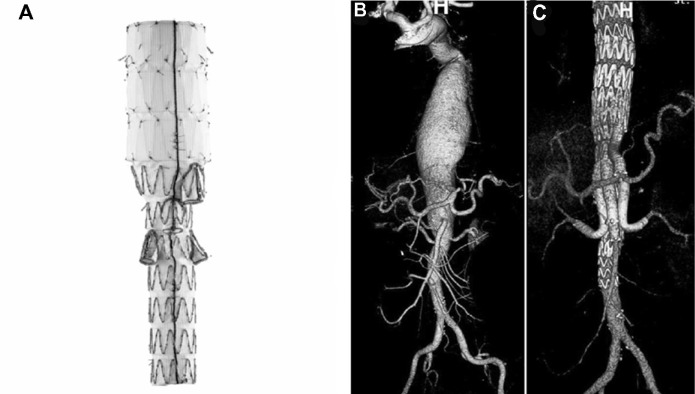
Branched endovascular devices. Notes: The Zenith t-Branch device (A) (Cook Medical, Bloomington, IN, USA) is designed with four downward projecting branched access limbs. It deploys via a preloaded 22-F delivery system. The superior mesenteric artery branch limb measures 8 mm wide by 18 mm long, and the celiac artery branch measures 8 mm wide by 21 mm long. The renal side branches measure 6 mm wide by 18 mm long. Above is an example of a complex aneurysm both before (B) and after (C) t-Branch endovascular treatment. Copyright © 2013 International Society of Endovascular Specialists. Reproduced from Bosiers MJ, Bisdas T, Donas KP, Torsello G, Austermann M. Early experience with the first commercially available off-the-shelf multibranched endograft (t-branch) in the treatment of thoracoabdominal aortic aneurysms. J Endovasc Ther. 2013;20(6):719–725.
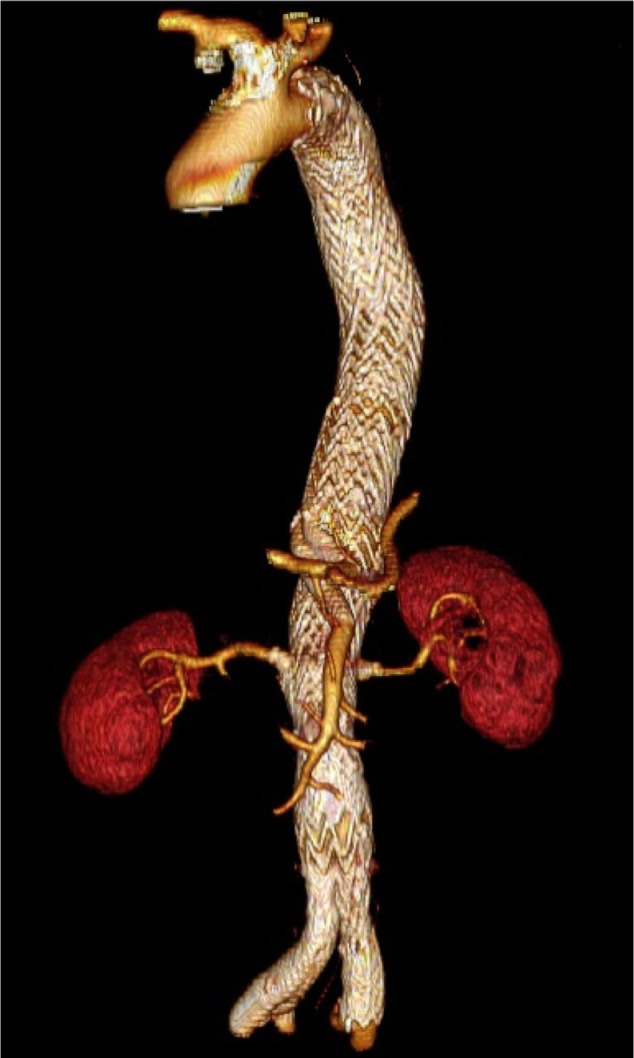
Parallel endografts. Notes: Postoperative three-dimensional volume rendering of a type II thoracoabdominal aneurysm treated with parallel endografts. The visceral stents were placed antegrade via left axillary access. The renal stents were placed retrograde via contralateral femoral access.
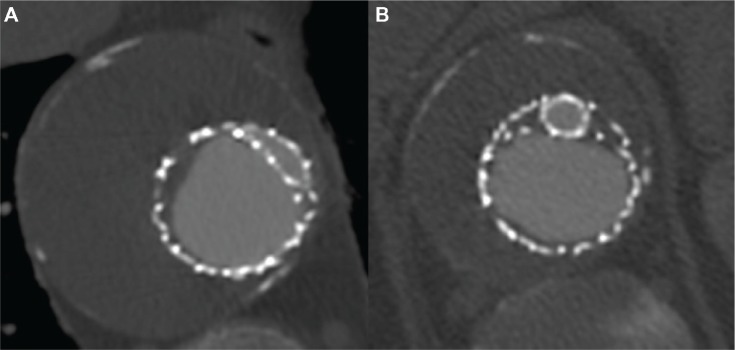
Molded TEVAR. Notes: Postoperative computed tomography scan of a type V thoracoabdominal aneurysm treated with a single parallel graft to the celiac artery. The parallel graft has been molded to an eye-shape more proximally in the overlap zone to allow for perfect apposition of the multiple endoprostheses and elimination of any potential gutters (A). The parallel graft remains round more distally in the overlap zone near the origin of the celiac artery. Note the large gutters (B) that would have likely resulted in an endoleak if this covered stent had not been molded to an eye-shape more proximally. Abbreviation: TEVAR, thoracic endovascular aneurysm repair.
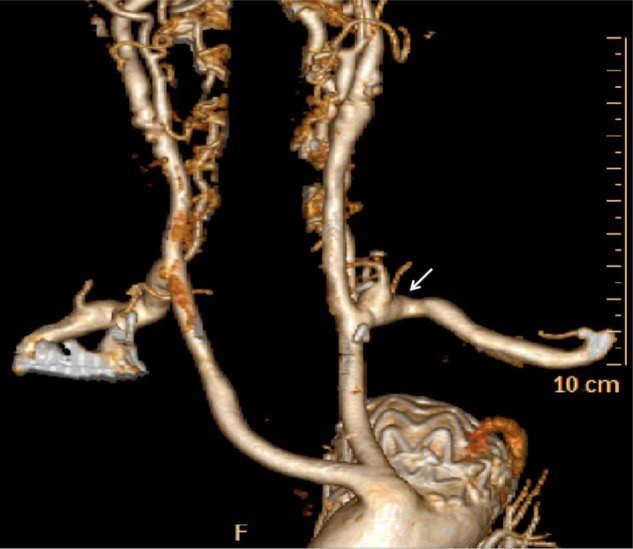
Arch debranching. Notes: Creation of a proximal landing zone can be accomplished with arch debranching. In this case, a left subclavian to left common carotid transposition (arrow) was created in anticipation of a Zone 2 proximal landing zone for subsequent TEVAR. Others have described the addition of carotid-carotid bypass to allow Zone 1 proximal landing zone creation. Abbreviation: TEVAR, thoracic endovascular aneurysm repair.
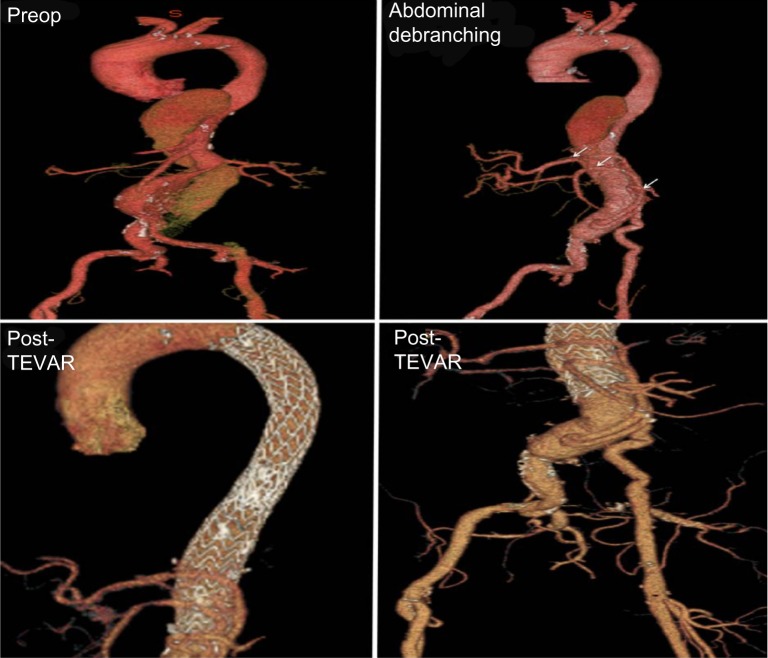
Multivisceral abdominal debranching. Notes: Creation of a distal landing zone can be accomplished with abdominal debranching procedures. Celiac, SMA, and either or both renal arteries (arrows) can be debranched to facilitate TEVAR landing zones. Recent introduction of hybridized grafts has simplified this procedure. In addition, in those patients with poor access vessel diameter, a conduit limb can be tunneled into the anterior abdominal wall and left in place for future exposure, thrombectomy, and controlled access for later TEVAR introduction. Abbreviations: Preop, preoperatively; SMA, superior mesenteric artery; TEVAR, thoracic endovascular aneurysm repair.
References
-
- Stein L, Elefteriades J. Epidemiology and natural history of thoraco-abdominal aortic aneurysms. In: Chiesa R, Melissano G, Zangrillo A, editors. Thoraco-Abdominal Aorta. Springer; Milan: 2011. pp. 25–32.
-
- Clouse WD, Hallett JW, Jr, Schaff HV, et al. Improved prognosis of thoracic aortic aneurysms: a population-based study. JAMA. 1998;280(22):1926–1929. - PubMed
-
- Knepper J, Upchurch GR. A review of clinical trials and registries in descending thoracic aortic aneurysms. Semin Vasc Surg. 2010;23(3):170–175. - PubMed
-
- Crawford ES, Coselli JS. Thoracoabdominal aneurysm surgery. Semin Thorac Cardiovasc Surg. 1991;3(4):300–322. - PubMed
-
- Safi HJ, Miller CC., 3rd Spinal cord protection in descending thoracic and thoracoabdominal aortic repair. Ann Thorac Surg. 1999;67(6):1937–1939. discussion 1953–1958. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
