

Addressing barriers to optimal oral anticoagulation use and persistence among patients with atrial fibrillation: Proceedings, Washington, DC, December 3-4, 2012
- PMID: 25173533
- PMCID: PMC4269555
- DOI: 10.1016/j.ahj.2014.04.007
Addressing barriers to optimal oral anticoagulation use and persistence among patients with atrial fibrillation: Proceedings, Washington, DC, December 3-4, 2012
Abstract
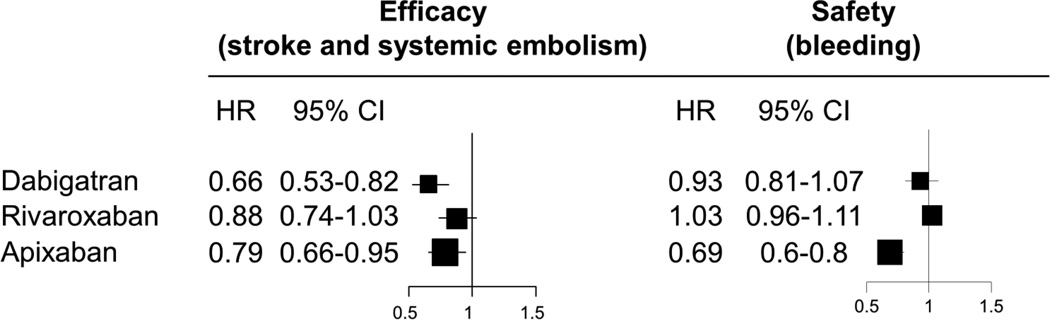
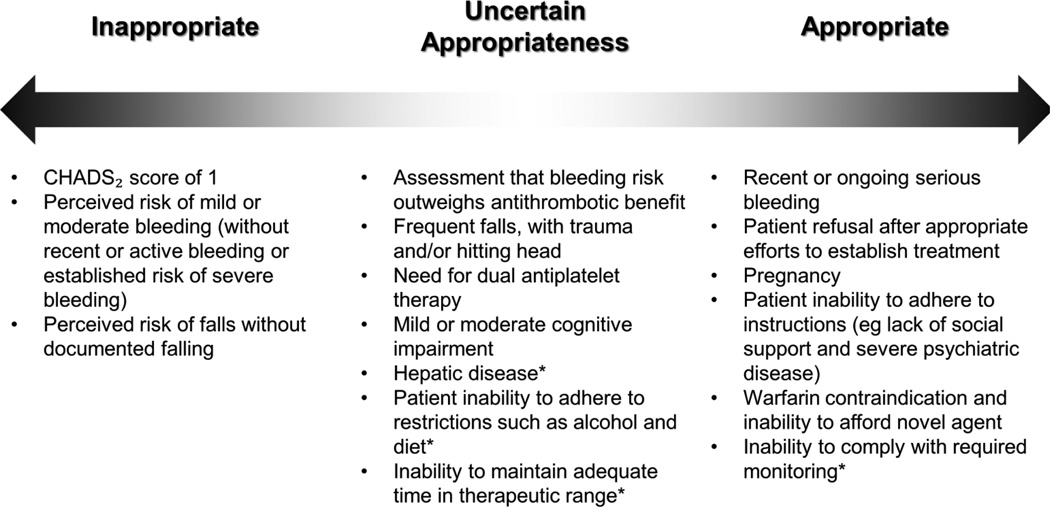
Approximately half of patients with atrial fibrillation and with risk factors for stroke are not treated with oral anticoagulation (OAC), whether it be with vitamin K antagonists (VKAs) or novel OACs (NOACs); and of those treated, many discontinue treatment. Leaders from academia, government, industry, and professional societies convened in Washington, DC, on December 3-4, 2012, to identify barriers to optimal OAC use and adherence and to generate potential solutions. Participants identified a broad range of barriers, including knowledge gaps about stroke risk and the relative risks and benefits of anticoagulant therapies; lack of awareness regarding the potential use of NOAC agents for VKA-unsuitable patients; lack of recognition of expanded eligibility for OAC; lack of availability of reversal agents and the difficulty of anticoagulant effect monitoring for the NOACs; concerns with the bleeding risk of anticoagulant therapy, especially with the NOACs and particularly in the setting of dual antiplatelet therapy; suboptimal time in therapeutic range for VKA; and costs and insurance coverage. Proposed solutions were to define reasons for oral anticoagulant underuse classified in ways that can guide intervention and improve use, to increase awareness of stroke risk as well as the benefits and risks of OAC use via educational initiatives and feedback mechanisms, to better define the role of VKA in the current therapeutic era including eligibility and ineligibility for different anticoagulant therapies, to identify NOAC reversal agents and monitoring strategies and make knowledge regarding their use publicly available, to minimize the duration of dual antiplatelet therapy and concomitant OAC where possible, to improve time in therapeutic range for VKA, to leverage observational data sets to refine understanding of OAC use and outcomes in general practice, and to better align health system incentives.
Copyright © 2014 Mosby, Inc. All rights reserved.
Figures
References
-
- Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults; national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk factors In Atrial fibrillation (ATRIA) study. JAMA. 2001;285:2370–2375. - PubMed
-
- Ogilvie IM, Newton N, Welner SA, et al. Underuse of oral anticoagulants in atrial fibrillation: a systematic review. Am J Med. 2010;123:638–645. - PubMed
-
- Piccini JP, Hernandez AF, Zhao X, et al. Quality of care for atrial fibrillation among patients hospitalized for heart failure. J Am Coll Cardiol. 2009;54:1280–1289. - PubMed
-
- Connolly SJ, Pogue J, Eikelboom J, et al. Benefit of oral anticoagulant over antiplatelet therapy in atrial fibrillation depends on the quality of international normalized ratio control achieved by centers and countries as measured by time in therapeutic range. Circulation. 2008;118:2029–2037. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
